Institution: Veterans Affairs Medical Center, Washington, DC; The George Washington University, Washington, DC
Additional authors:Min-Ling Lui, MD, PhD
Session: AML with myelodysplasia-related changes
HISTORY
The patient is a 63-year-old African American man and Vietnam War veteran with history of Agent Orange exposure and no prior history of cancer. Two years prior to the diagnosis of acute myeloid leukemia, he presented with shortness of breath and fatigue. Complete blood counts revealed anemia and neutropenia. Bone marrow biopsy showed hypercellular marrow with trilineage dysplasia and diffuse marrow fibrosis (grade 1-2 of 3). There was no increase in blasts (<1%) and the karyoptype was 46, XY. The findings were consistent with myelodysplastic syndrome (refractory cytopenia with multilineage dysplasia, RCMD), with fibrosis.
The patient was initially managed with erythropoietin. Although transfusion independent, his peripheral blood counts continued to decline. Six months after presentation, he was pancytopenic and was treated with five cycles of 5-azacytidine. Following chemotherapy, his reticulocyte count increased (5%), but his peripheral blood started to show markedly elevated numbers of nucleated red blood cells (>150 per 100 white blood cells), many dysplastic. Bone marrow biopsy demonstrated hypercellularity with trilineage dysplasia and marked megakaryocyte hyperplasia. Elevated myeloblasts (10%) were identified in the peripheral blood and marrow aspirate smears, and confirmed by flow cytometric analysis. The karyotype was normal. The findings were consistent with myelodysplastic syndrome, refractory anemia with excess blasts (RAEB-2).By this time, the patient was transfusion dependent, with severe neutropenia and thrombocytopenia. He was given three cycles of lenalidomide. A subsequent bone marrow biopsy revealed persistent trilineage dysplasia with 15% blasts. The patient was treated with three cycles of 5-aza-2-deoxycytidine. Following the third cycle of chemotherapy, the patient was admitted to hospital for neutropenic fever. Imaging on admission revealed a large pericardial effusion. Flow cytometric analysis on the pericardiocentesis revealed 32% blasts. Bone marrow aspirate and core biopsy confirmed transformation into acute myeloid leukemia.DETAILS
A trephine core biopsy of the posterior iliac crest was received in neutral formalin along with air-dried touch preparations. The touch preparations were stained by the Wright-Geimsa method. The core biopy was further fixed in B5 fixative, decalcified, and processed for routine sectioning.
The bone marrow biopsy was hypercellular (100%) with trilineage hyperplasia. The megakaryocytes were markedly increased in number with extensive cohesive clustering. They were left shifted and dysplastic with polymorphism, multinucleation, and hyperchromasia. The myeloid to erythroid ratio was 1-2:1. The myeloid lineage was markedly left shifted, with increased numbers of large, immature cells, singly and in clusters showing high nuclear to cytoplasmic ratio, vesicular chromatin and prominent nucleoli. Myelofibrosis was evaluated using a reticulin stain that revealed extensive marrow fibrosis with a diffuse, coarse fiber network (grade 3 of 3).No aspirate smears were received due to a “dry tap”. Touch preparations of the core biopsy showed many blasts with a high nuclear to cytoplasmic ratio, fine chromatin, and nucleoli. A manual differential showed 26% blasts, 24% myeloid precursors, 0% neutrophils/bands, 36% erythroid precursors, and 14% lymphocytes.The peripheral blood smear showed pancytopenia with circulating blasts. Red blood cells displayed mild to moderate anisopoikilocytosis with teardrop cells, polychromasia and numerous nucleated red blood cells (136 nucleated red blood cells per 100 white blood cells). The white blood cells were markedly left shifted. A manual cell count provided 20% blasts, 11% more mature granulocytes, 14% monocytes, 55% lymphocytes.IMMUNOHISTOCHEMISTRY AND FLOW CYTOMETRY
Immunohistochemical staining of the core biopsy for CD34 and CD117 highlighted about 20%of the morphologically immature cells. CD61 stained numerous megakaryocytes (40%), many dysplastic, some immature appearing and co-expressing CD34. MPO and Glycophorin-A demonstrated a myeloid to erythroid ratio of about 1-2:1.
Flow cytometric analysis was performed on a hemodiluted aspirate attempt. Markers included CD13, CD14, CD22, CD33, CD34, CD41, CD61, CD117, HLA-DR, TdT, kappa, lambda, and glycophorin-A. Viability was suboptimal at 80%. CD45 (dim) positive blasts accounted for 36% of the total viable cells. The blasts were positive for CD34, CD33, CD13, HLA-DR, CD117, CD11c, CD7 (dim), and TdT (subpopulation), consistent with myeloblasts. They were negative for CD41, CD61 and glycophorin-A.CYTOGENETIC FINDINGS
The karyotype at final diagnosis was 47, XY, +8.
MOLECULAR FINDINGS
Negative for the FLT3 internal tandem duplication and for the FLT3 D835 variant.
INTERESTING FEATURES
The case is that of a well documented antecedent myelodysplastic syndrome transforming into an acute myeloid leukemia. The patient presented with MDS-RCMD of the intermediate-risk group, without cytogenetic abnormality or increased blasts. However, at the initial diagnosis, his marrow demonstrated mild to moderate diffuse myelofibrosis. Significant myelofibrosis is unusual and has only been reported in a minority of MDS patients, usually in patients with excess blasts, and is associated with an aggressive clinical course.
As his disease evolved into acute leukemia, the marrow was remarkable for the degree of megakaryocytic hyperplasia and dysplasia, as highlighted by immunohistochemisty, which demonstrated dysplastic megakaryocytes often forming large aggregates associated with clusters of immature cells, some coexpressing CD34 and CD61, raising the possibility of transformation into an acute megakaryoblastic leukemia. However, on cytologic evaluation of the peripheral blood and hemodilluted aspirate specimens, the blast morphology was largely undifferentiated with no evidence of megakaryocytic differentiation. Flow cytometric analysis confirmed that most of the blasts were myeloblasts, without megakaryocytic differentiation, positive for CD34, CD117, CD13, and CD33, and negative for CD41 and CD61. The presence of extramedullary disease has been documented, and though conclusive evidence is not available in this case, the clinical and laboratory findings indicate possible pericardial involvement. Interestingly, the patient’s cytogenetics were normal up until the time of transformation, when trisomy of chromosome 8, an abnormality associated with poorer prognosis, was identified. Molecular studies of the FLT3 gene were noncontributory.PROPOSED DIAGNOSIS
The findings are consistent with acute myelogenous leukemia transforming from myelodysplastic syndrome.
CONSENSUS DIAGNOSIS
Acute myeloid leukemia with myelodysplasia-related changes, with prominent megakaryocytic/megakaryoblastic differentiation
| IMAGE 1 - Findings at the diagnosis of myelodysplastic syndrome, refractory anemia with excess blasts (RAEB-2); Bone Marrow Biopsy, 400X; Hypercellular and left shifted marrow with dysplastic megkaryocytes. | 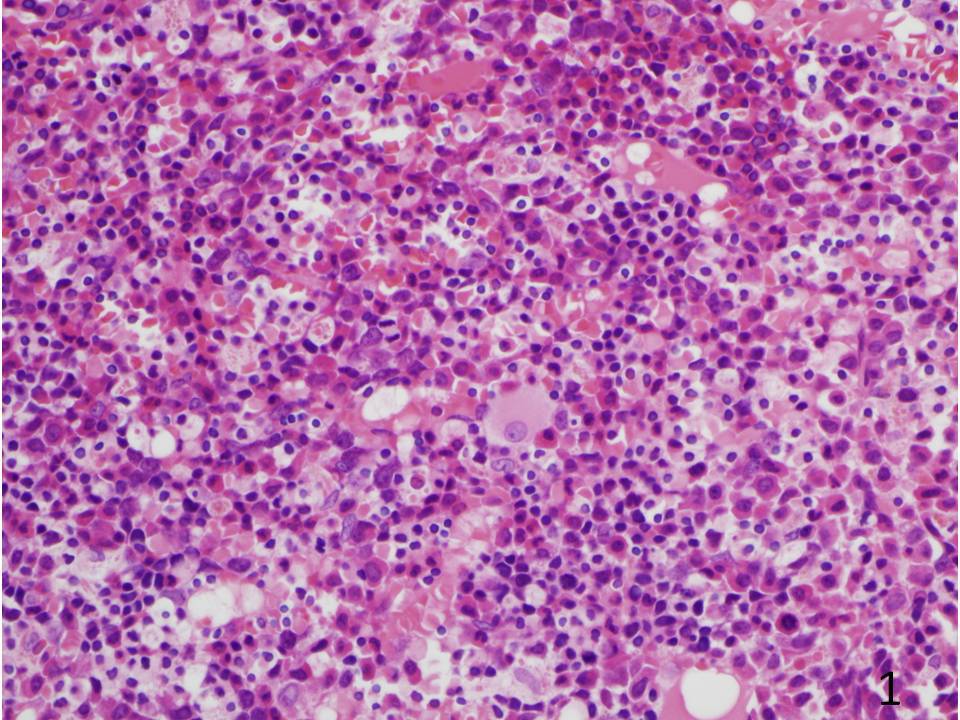 |
| IMAGE 2 - Findings at the diagnosis of myelodysplastic syndrome, refractory anemia with excess blasts (RAEB-2); Bone Marrow Aspirate; Dysgranulopoiesis with hypogranulation, hypersegmentation and pseudo Pelger-Huet cells. Dyserythropoiesis with bi-/multi-nucleation, protrusions, bridging and megaloblastoid changes. |  |
| IMAGE 2 - Findings at the diagnosis of myelodysplastic syndrome, refractory anemia with excess blasts (RAEB-2); Bone Marrow Aspirate; Dysgranulopoiesis with hypogranulation, hypersegmentation and pseudo Pelger-Huet cells. Dyserythropoiesis with bi-/multi-nucleation, protrusions, bridging and megaloblastoid changes. |  |
| IMAGE 4 - Findings at transformation; Bone Marrow Biopsy, 40X. |  |
| IMAGE 5 - Findings at transformation; Bone Marrow Biopsy, 200X. |  |
| IMAGE 6 - Findings at transformation; Bone Marrow Biopsy, 400X. |  |
| IMAGE 7 - Findings at transformation; Reticulin Stain, 400X. |  |
| IMAGE 8 - Findings at transformation; Immunohistochemical stains. |  |
| IMAGE 9 - Findings at transformation; Bone Marrow Touch Prep, 1000X. |  |
| IMAGE 10 - Findings at transformation; Peripheral Blood, 1000X; Blasts. | 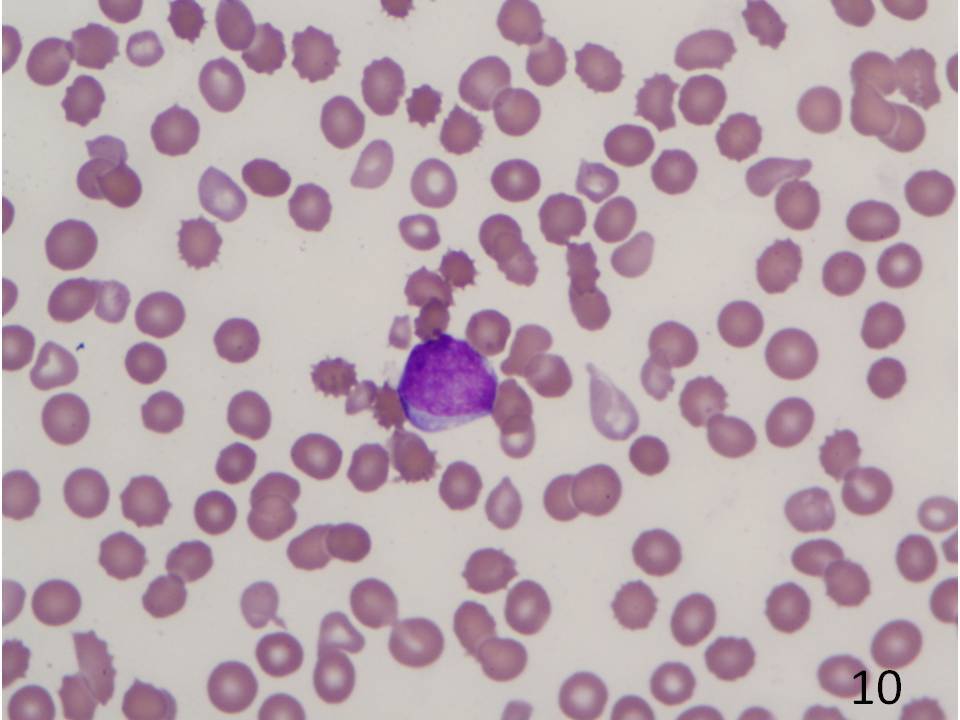 |