Institution: University of Michigan
Additional authors:Harry P. Erba, MD, PhD; Dale L. Bixby, MD, PhD; Diane Roulston, PhD
Session: AML with recurrent genetic abnormalities Part I
HISTORY
A 34-year-old woman presented with mild facial cellulitis (promptly resolved with oral antibiotics) and acute onset fever, chills, and headache. CBC data at presentation included: WBC 1900/uL (absolute neutrophil count 900/uL); Hb 10.7 g/dL; MCV 97 fL; and platelet count 314,000/uL. The peripheral blood contained about 20% blasts. The blood and bone marrow morphology were consistent with acute myeloid leukemia (AML) with inv(3); RPN1-EVI1, confirmed by cytogenetic analysis.
AML with the recurrent genetic abnormality inv(3) is associated with a younger age at diagnosis, resistance to standard induction chemotherapy, and a very poor long-term prognosis. Better therapeutic strategies are sorely needed. As such, it was decided to employ a new induction chemotherapy strategy of concurrent azacitidine and lenalidomide (see references below). The induction course was uncomplicated and she required hospitalization only for the first 7 days of treatment. No red cell or platelet transfusions were required during the entire course of therapy (five cycles over 21 weeks). Bone marrow examination at day #21 of therapy documented a low level of persistent leukemia. Bone marrow examination at day #49 (after 2 cycles of the same therapy) documented complete remission (morphologic, flow cytometric, and cytogenetic). Plans for allogeneic stem cell transplant were made but the transplant was delayed for psychosocial reasons.Bone marrow examination at week #21 (after 5 cycles of azacitidine/lenalidomide) revealed morphologic evidence of early relapse (4.8% blasts in bone marrow with abnormal megakaryocytes), confirmed by cytogenetics in 2 of 20 cells. Four weeks later she underwent allogeneic peripheral blood stem cell transplant from a sibling donor.DETAILS
Bone marrow trephine core biopsy (AZF fixation) taken from left ilium at time of initial presentation. The bone marrow was hypocellular (20% cellularity) with 25% myeloblasts, increased megakaryocytes, and a normal granulocytic:erythroid ratio. The blasts were of variable size with sparse cytoplasmic granulation. No Auer rods were found. Megakaryocytes were distributed singly and in clusters, with prominent dysmegakaryopoiesis including many small forms with nuclear hypolobation. Peripheral blood findings included leukemic myeloblasts, absolute neutropenia with pelgeroid dysmorphology, and a normal platelet count with dysmorphic platlelets (some large and hypogranular forms).
IMMUNOHISTOCHEMISTRY AND FLOW CYTOMETRY
Immunohistochemical stains for CD34 and CD117 were performed on sections of the core biopsy; these highlighted the increased blasts (20-30%) distributed interstitially and in clusters.
Flow cytometric immunophenotyping of the peripheral blood blasts documented expression of CD11c (dim), CD13 (dim), CD33 (dim), CD34 (bright), CD38 (dim), CD45 (dim), CD117 (dim), and CD5 (dim, in a minor subset). The blasts were negative for CD2, CD3, CD7, CD10, CD14, CD19, CD20, CD22, and CD56.CYTOGENETIC FINDINGS
45,XX,inv(3)(q21q26.2),-7 in 13 of 20 cells analyzed from the bone marrow.
MOLECULAR FINDINGS
Bone marrow was negative for all mutations tested, including: FLT3 ITD; FLT3 D835; NPM1 exon 12; CEPBA; KIT D816V; IDH1 codon 132; IDH2 codons 140, 172.
INTERESTING FEATURES
An illustration of the typical morphologic features of this uncommon subtype of acute myeloid leukemia. Remission was achieved using new therapeutic agents (azacitidine and lenalidomide), with a durable response in preparation for subsequent allogeneic stem cell transplantation. Furthermore, the pre-transplant therapy was given almost entirely on an outpatient basis and required no transfusion support.
References:1. Sekeres MA et al. Phase 2 study of the lenalidomide and azacitidine combination in patients with higher-risk myelodysplastic syndromes. Blood. 2012 Dec 13;120(25):4945-51.2. Ramsingh G et al. A phase 1 study of concomitant high-dose lenalidomide and 5-azacitidine induction in the treatment of AML. Leukemia. 2012 Jul 25. doi: 10.1038/leu.2012.214. [Epub ahead of print]3. Pollyea DA et al. Safety, efficacy and biological predictors of response to sequential azacitidine and lenalidomide for elderly patients with acute myeloid leukemia. Leukemia. 2012 May;26(5):893-901.PROPOSED DIAGNOSIS
Acute myeloid leukemia with recurrent genetic abnormality, inv(3)(q21q26.2); RPN1-EVI1.
CONSENSUS DIAGNOSIS
Acute myeloid leukemia with inv(3)(q21q26.2); RPN1-EVI1, and -7
| bone marrow biopsy, H&E; abnormal megakaryocytes and increased blasts | 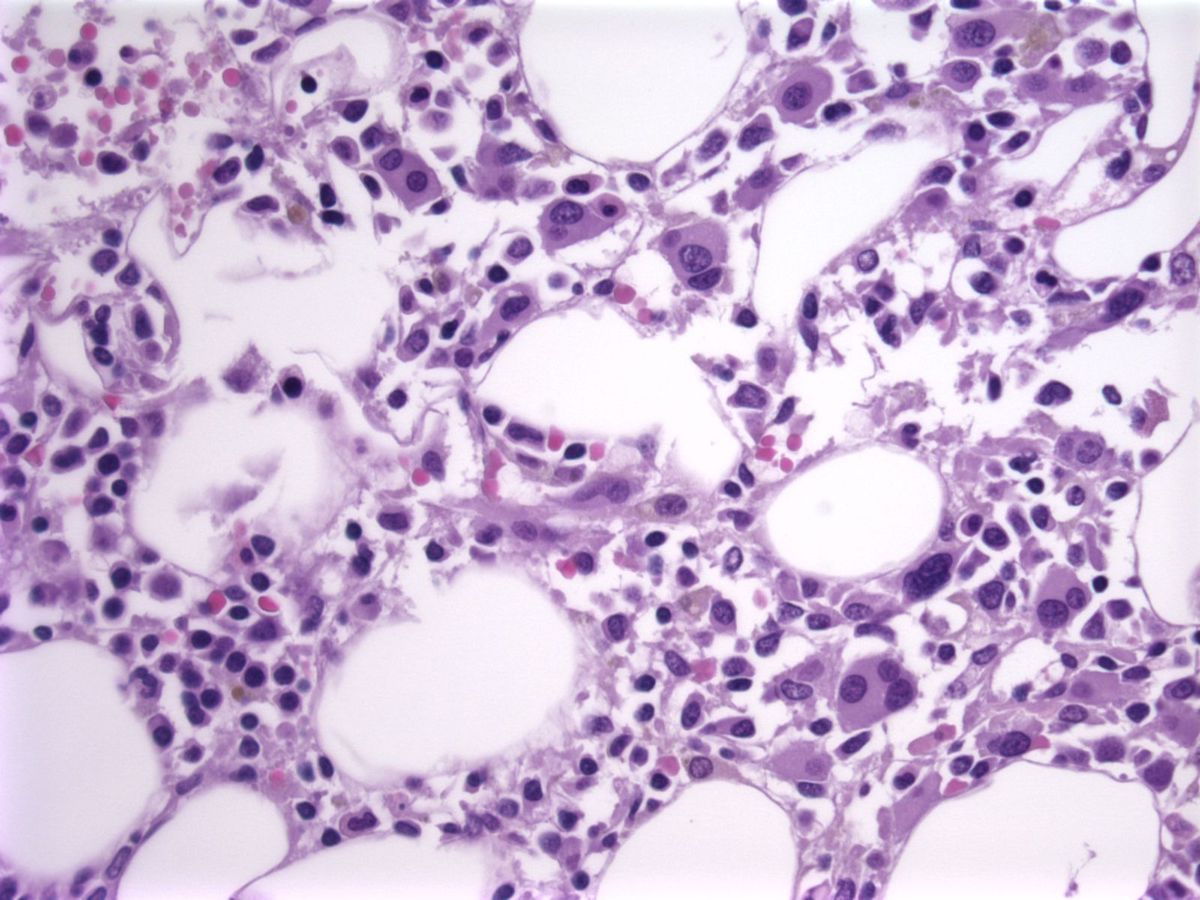 |
| bone marrow biopsy, H&E; abnormal megakaryocytes and increased blasts | 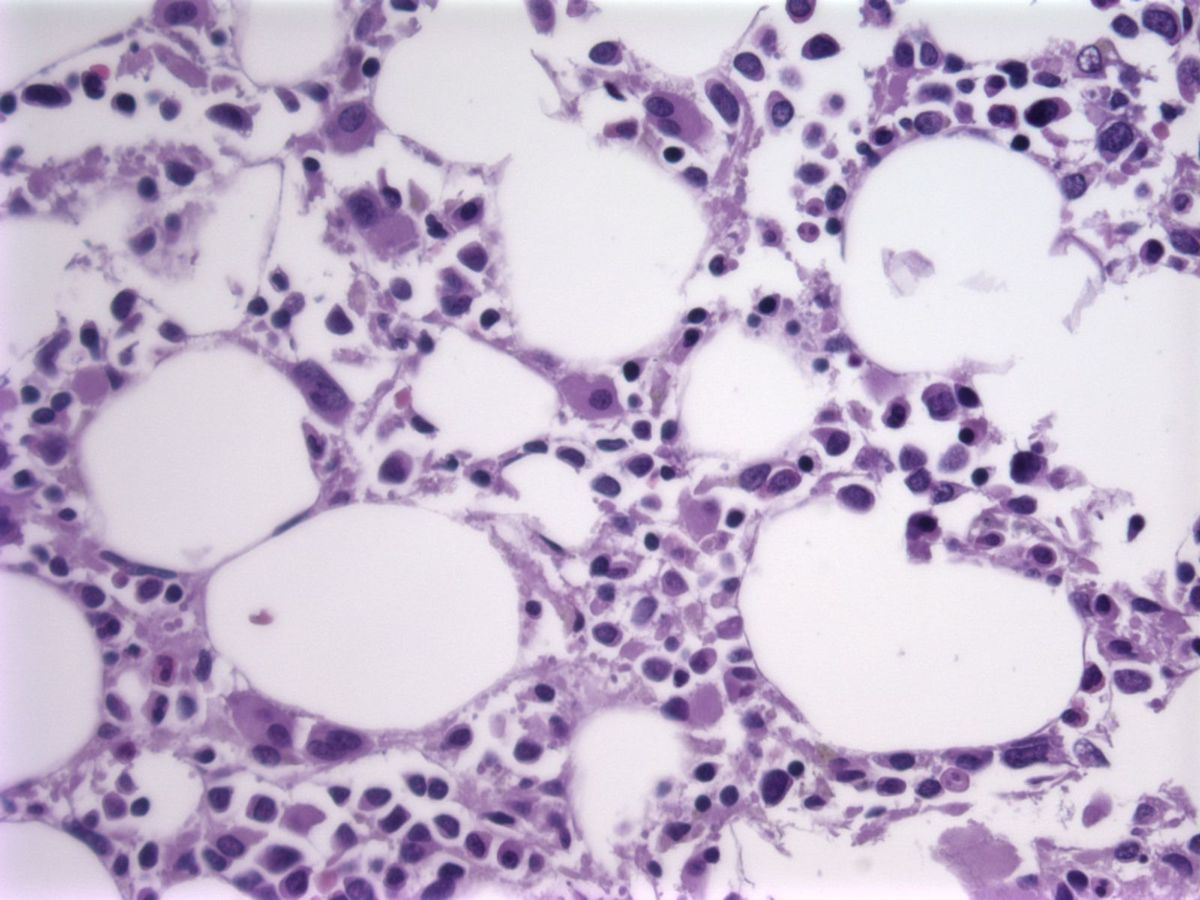 |
| CD34, bone marrow biopsy | 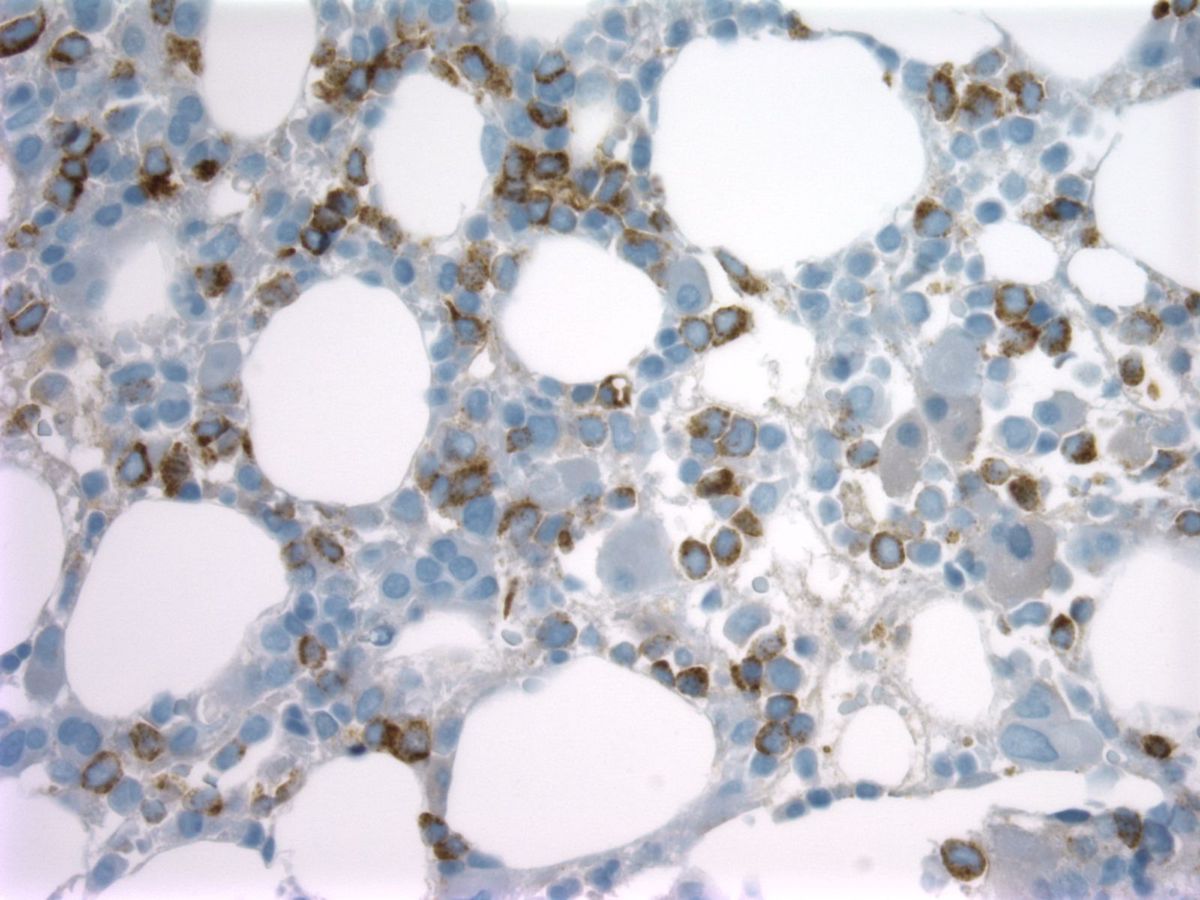 |
| CD117, bone marrow biopsy |  |
| myeloblast, bone marrow aspirate smear | 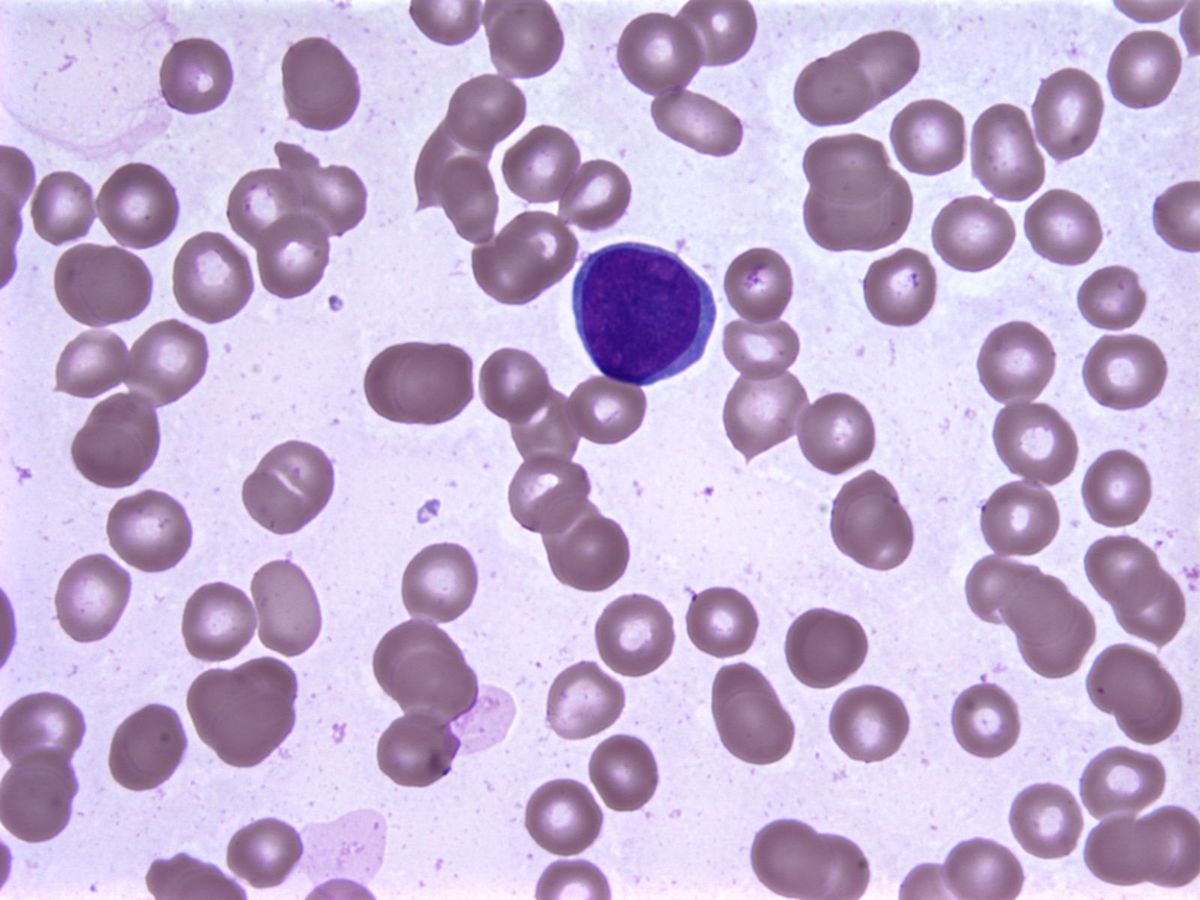 |
| myeloblast, bone marrow aspirate smear |  |
| bone marrow karyogram; 45,XX,inv(3)(q21q26.2),-7 |  |
| myeloblast, peripheral blood smear |  |
| dysmorphic platelet, peripheral blood smear |  |
| hypogranular platelets, peripheral blood smear |  |
| pelgeroid neutrophil, peripheral blood smear |  |
| pelgeroid neutrophil, peripheral blood smear |  |