Institution: University of New Mexico Health Sciences
Additional authors:Mohammad A. Vasef, Cristhiam Rojas-Hernandez
Session: Extramedullary manifestations of myeloid neoplasms
HISTORY
A 56-year-old male was admitted with a 3-4 days history of a constant, stabbing, epigastric abdominal pain, associated with numbness and tingling involving the entire circumference of the lower extremities, from hips to feet, and subjective weakness in this distribution. His past medical history included a JAK2-positive myeloproliferative neoplasm classified as polycythemia vera in 1996 and treated with hydroxyurea and splenectomy in 2002.
A current CBC revealed a white blood cell count of 15 x 10^6 cells/L with 82% neutrophils, 10% lymphocytes, 6% monocytes, and 2% eosinophils, a hemoglobin of 14 g/dL and a markedly elevated platelet count of 957 x 10^6 /L. MRI of the entire spine demonstrated cord compression due to a posterior and right lateral epidural mass starting at the T4-5 level and extending to the inferior T9 level. In addition, an L3 mass with extra osseous extension was also detected with moderate spinal canal stenosis as well as severe right L2-L3 neural foraminal stenosisDETAILS
Review of the bone marrow biopsy from 1996 showed a hypercellular marrow (70%) with panmyelosis including increased highly atypical megakaryocytes with bulbous, hyperlobated, and hyperchromatic nuclei with frequent clustering.
The splenectomy specimen from 2002 weighed 356 gram with unremarkable with intact histomorphologic features and without significant extramedullary hematopoiesis.Debulking of the spinal mass was performed and portions of fresh specimen were sent for flow cytometric immunophenotyping and cytogenetic analysis. Representative tissue was fixed in neutral formalin and processed for routine morphologic evaluation.The histologic sections demonstrated diffuse proliferation of atypical cells with degenerative features and small foci of necrosis. The atypical cells in relatively preserved foci were predominantly composed of large cells with hyperchromatic round nuclei, prominent nucleoli, and moderate amounts of amphophilic cytoplasm. Mitotic figures were easily identified.A concurrent bone marrow biopsy revealed a hypercellular marrow (80-90%) with markedly increased atypical megakaryocytes with prominent and extensive clustering, and with a spectrum of morphology including predominance of bizarre forms with bulbous nuclei and high N:C ratio and subsets of hyperchromatic, bare, and hyperlobated nuclei. No increased blasts or abnormal infiltrate reminiscent of those observed in spinal mass excision was identified in bone marrow specimen. A reticulin stain revealed only a mild increase in reticulin fibrosis (1+).IMMUNOHISTOCHEMISTRY AND FLOW CYTOMETRY
Flow cytometry on the spinal mass demonstrates approximately 25% of events to be large, complex cells expressing CD4, CD13, CD14, CD33, CD36, CD64, HLA-DR, dim CD7, and dim CD117.
Flow cytometry on the concurrent bone marrow showed 2% of events to be blasts with CD34, dim CD45, and CD33. There was no abnormal population with immunophenotypic features of those detected in spinal mass was identified. By paraffin immunohistochemistry, the neoplastic cells in spinal tumor expressed CD4, CD33, CD43, CD45, CD71, CD30 (blush), and EMA. Immunostain for Ki-67 demonstrated a proliferation index estimated at 80%. The neoplastic cells were negative for CD3, CD5, CD7, CD8, CD19, CD20, CD31, CD34, CD42b, CD56, CD68, CD79a, CD117, CD123, CD138, CD163, hemoglobin A, myeloperoxidase, lysozyme, kappa, lambda, TIA1, S100, vimentin, CAM 5.2, and cytokeratin AE1/AE3. EBER stain showed no EBV-infected cells.CYTOGENETIC FINDINGS
Cytogenetic findings on the spinal mass:
41~46,X,Y,+1,+2,add(5)(p15),+6,t(9;18)(p10;p10), add(10)(q24),add(11)(p15),-13,-14,+del(16)(q21),+21,-22,-22[cp3]/ 46,XY[17]Cytogenetic findings on the current bone marrow: 46,XY[20]MOLECULAR FINDINGS
JAK2 V617F mutation was detected in the spinal lesion and bone marrow biopsy using an allelic discrimination, PCR based assay. The bone marrow was negative for BCR/ABL1 fusion transcripts by quantitative real time PCR.
INTERESTING FEATURES
Myeloid sarcoma presenting as a spinal mass with cord compression in the setting of non-CML MPN in non-leukemic phase is rare and only sporadic cases have been previously reported. Our case represents a unique example of the accumulation of multiple chromosomal abnormalities in a JAK2 V617F-positive MPN that transformed to JAK2 V617F-positive myeloid sarcoma that could have led to the aggressive and treatment-refractory behavior of this patient’s disease.
PROPOSED DIAGNOSIS
Myeloid sarcoma, JAK2 V617F-positive, arising in a JAK2 V617F-positive non-CML myeloproliferative neoplasm
CONSENSUS DIAGNOSIS
Blast phase of JAK2 V617F-positive myeloproliferative neoplasm involving spinal masses (myeloid sarcomas)
| H&E-stained bone marrow core biopsy from 1996 | 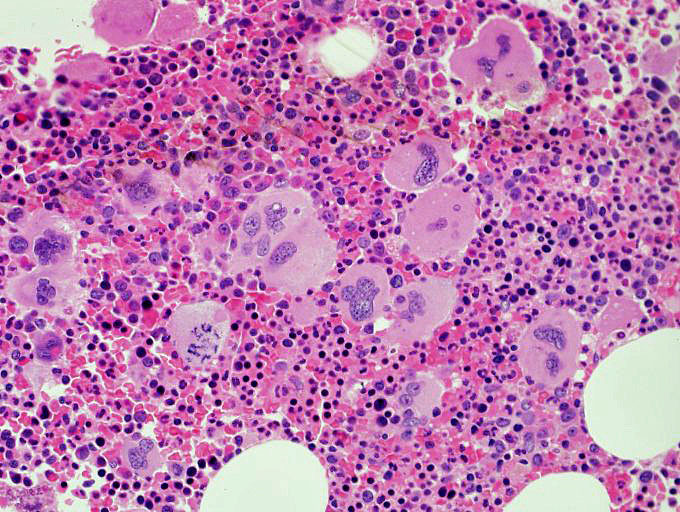 |
| H&E-stained section of spleen removed in 2002 showing unremarkable histomorphology with no significant extramedullarly hematopoiesis |  |
| H&E-stained section of spinal mass showing undifferentiated neoplastic cells with large nuclei with prominent nucleoli, and moderate amounts of amphophilic cytoplasm. Numerous mitoses are present in the background. |  |
| Flow cytometry of spinal mass showing an immature population expressing CD117, CD13, and HLA-DR (red) |  |
| Immunohistochemical stain for CD43 on spinal mass |  |
| Immunohistochemical stain for CD71 on spinal mass |  |
| Immunohistochemical stain for CD33 showing positivity in subset of neoplastic cells in spinal mass |  |
| Karyogram of spinal mass showing complex cytogenetic abnormalities | 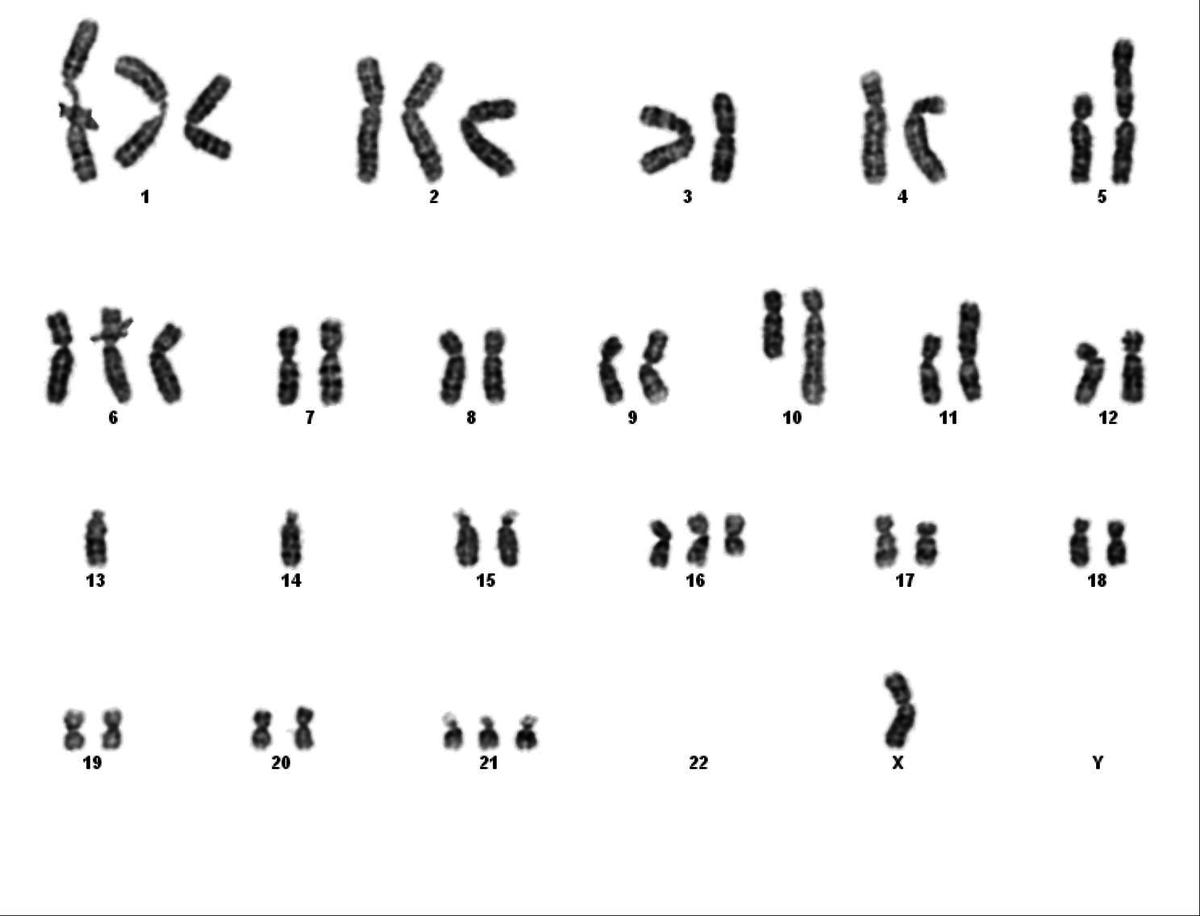 |
| H&E-stained bone marrow core biopsy from 2012 demonstrating morphologic findings similar to those noted in original bone marrow from 1996 |  |