Institution: University of Pennsylvania
Additional authors:Jennifer Morrissette PhD, Adam Bagg MD
Session: Therapy-related myeloid neoplasms
HISTORY
A 41-year-old female was diagnosed with moderately differentiated invasive ductal carcinoma of the right breast in January 2012. She was treated with bilateral mastectomies in February 2012, 6 cycles of adjuvant chemotherapy (docetaxel/Taxotere, cyclophosphamide, and trastuzumab/Herceptin), adjuvant radiation therapy and tamoxifen. In November 2012, she reported feeling “very tired” with a mild cough and sore throat. A CBC demonstrated WBC 7.4 x 103/L (5% neutrophils, 16% lymphocytes, 79% blasts), Hgb 10.2 g/dL, platelets 21 x 103/L. The blasts had large round to oval nuclei, fine chromatin, prominent nucleoli, and variable amounts of basophilc cytoplasm with salmon pink granules with infrequent obvious Auer rods.
Clinically, the patient completed induction chemotherapy with idarubicin and cytarabine and had a nadir marrow on 12/2012 that was chemoablated with no evidence of AML. The patient had a follow-up bone marrow biopsy on 1/2/13 with documented complete remission. She then underwent 4 cycles of consolidation with HiDAC therapy that completed in May 2013. Another bone marrow biopsy has not yet been performed.DETAILS
Bone marrow core biopsy: 1.6 cm x 0.2 cm, fixed in B5.
Normocellular marrow (60%) with an expansion of blasts (>90%). Marked decrease in normal trilineage hematopoietic elements. Aspirate smear: Hemodilute and without spicules. Blasts accounted for >90% of total cellularity. Myeloid precursors showed limited maturation (<10%). Marked decrease in normal trilineage hematopoietic elements, without overt dysplasia.IMMUNOHISTOCHEMISTRY AND FLOW CYTOMETRY
Peripheral blood flow cytometry:
Dominant blast immunophenotype: CD34+ CD117+ HLA-DR+ MPO+ with dim/variable expression of CD2, CD4, CD7, CD13, CD15, CD19, CD33, and CD64.Immunohistochemistry:Not performed.CYTOGENETIC FINDINGS
Bone marrow: 47,XX,t(8;21)(q22;q22),del(9)(q13q22),+der(21)t(8;21) [20]
MOLECULAR FINDINGS
Multiplex RT-PCR analysis on peripheral blood was positive for an RUNX1-RUNX1T1/ t(8;21) fusion transcript.
No mutations in KIT were identified.INTERESTING FEATURES
The development of an AML following chemo/radiotherapy supports a consideration of a therapy-related myeloid neoplasm (TRMN), and t(8;21) is well described in this setting. This translocation is typically associated with the use of topoisomerase II inhibitors, and a relatively short interval between therapy and the development of leukemia.
However, in this case:1) No topoisomerase II inhibitors were used (although an alkylating agent was)2) The interval is shorter than that described in the literature for therapy-related t(8;21)-AML (9 months in this case vs median of 37 months); and 3)An associated del(9q) is well-described and quite frequent in the setting of de novo t(8;21)-AML, but apparently not described in therapy-related t(8;21)-AML.Hence, is this indeed a TRMN t(8;21)-AML or pure coincidence, with a de novo t(8;21)-AML? This is prognostically (and thus therapeutically) relevant, given the quite different prognoses.PROPOSED DIAGNOSIS
De novo t(8;21)-positive AML (rather than therapy-related t(8;21)-AML (TRMN), despite the therapeutic context).
CONSENSUS DIAGNOSIS
Therapy related myeloid neoplasm, acute myeloid leukemia with t(8;21)
| Bone marrow aspirate - 100x | 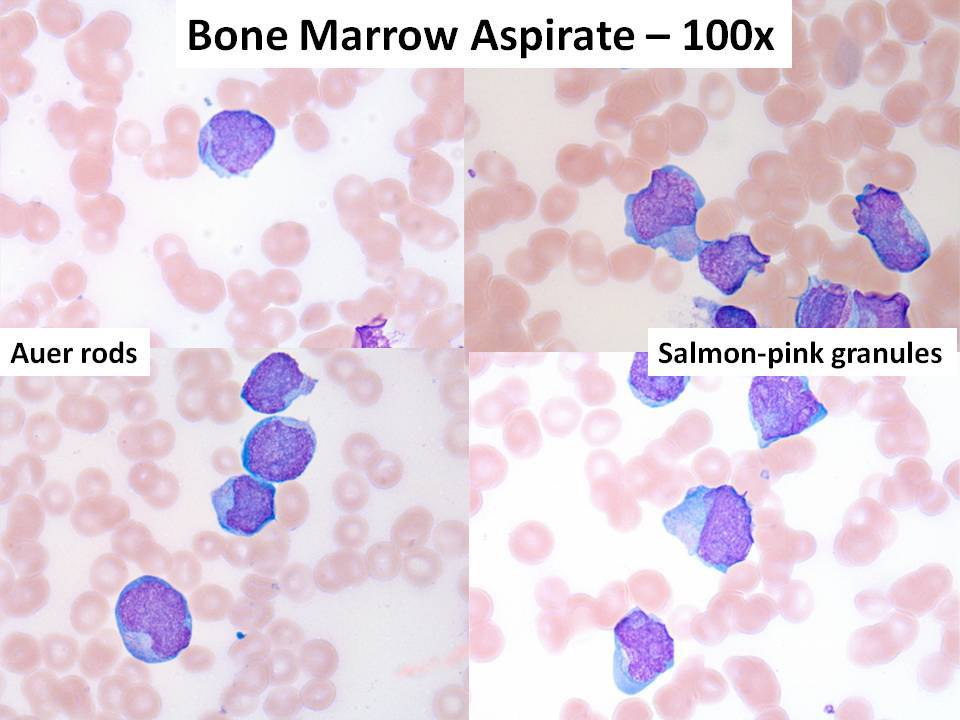 |
| Flow cytometry | 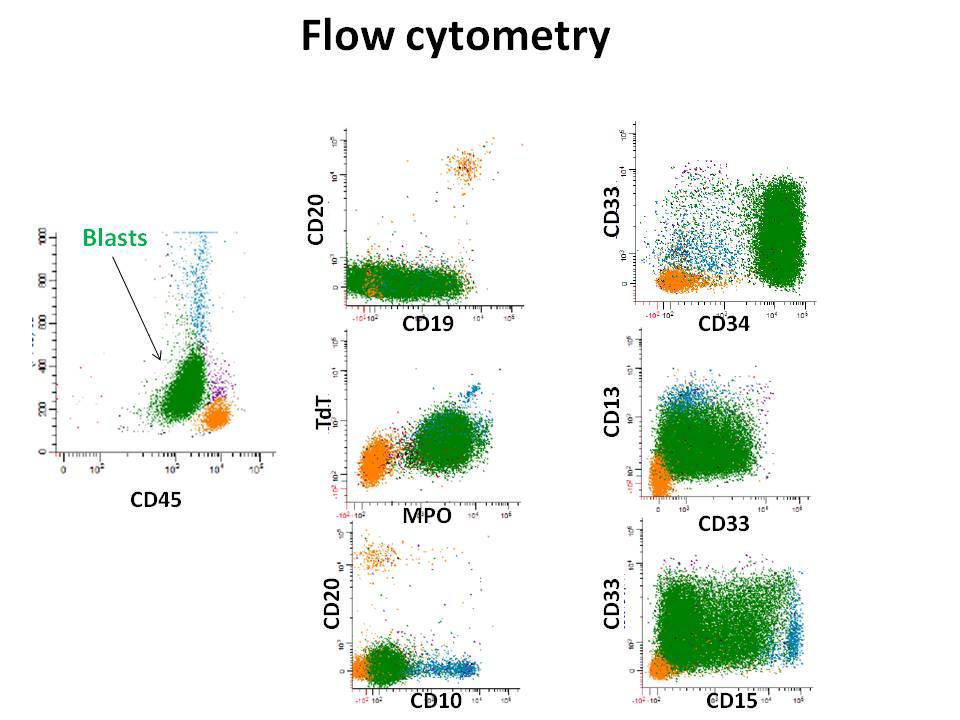 |
| Cytogenetics | 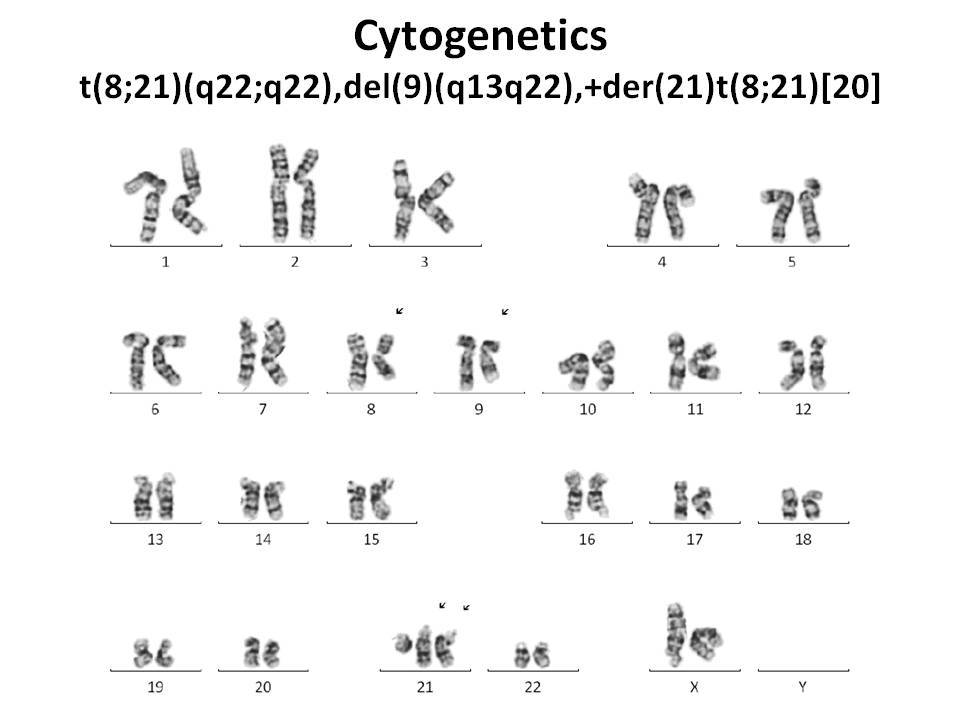 |