Institution: Department of Pathology, United Health Services Hospitals, Johnson City, NY
Additional authors:Robin Eastman-Abaya, MD (2) Melissa Anderson, BS (3) Joseph Readling, MD (4) Steven Gersen, PhD3) 2. Department of Pathology, Our Lady of Lourdes Hospital, Binghamton, NY 3. AmeriPath Northeast, Shelton, CT 4. Broome Oncology, Johnson City/Binghamton, NY
Session: Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB, or FGFR1
HISTORY
61-year-old female presented with rapidly growing mediastinal mass and diffuse peripheral lymphadenopathy, fevers and night sweats. Right inguinal lymph node biopsy done (A). A portion of lymph node was sent for flow cytometric analysis. She was treated for the disease diagnosed in the lymph node. Peripheral blood smear and a bone marrow core biopsy with touch imprints were performed as a part of staging work-up (B). Six months after the lymph node biopsy, another bone marrow biopsy was done because of the appearance of numerous blasts in the peripheral blood and marked thrombocytopenia at 17K/uL (C). She was treated for the disease detected in her bone marrow. She died a few days after the treatment was started.
DETAILS
A. Lymph node: DiffQuik-stained touch imprints showed many blastic cells with high N/C ratio and infrequent nucleolar prominence and a few eosinophils and eosinophil presursors. H and E sections showd small to medium-sized blastic cells with high N/C ratio, numerous mitoses, richness of high endothelial cell venules, and a few eosinophils and eosinophil precursors.
B. Peripheral Blood and First Bone Marrow: Peripheral blood showed mild absolute eosinophilia and mild absolute basophilia. Bone marrow touch inprints showed about 2% blasts, markedly increased eosinophils, eosinophil precursors and increased basophils. Bone marrow core biopsy showed a few areas with sheets of eosinophils and eosinophil precursors and large areas of marked reticulin fibrosis. Megakaryocytes (small and large) were increased.C. Peripheral Blood and Second Bone marrow: Peripheral blood showed numerous blasts. Bone marrow showed approximately 85% large blasts with, moderate N/C raio, prominent nucleoli, and large amount of blue/vacuolated cytoplasm (i.e monoblastic appearance). Core biopsy sections showed sheets of large blasts with moderate N/C raio and prominent nucleoli. Marked reticulin fibrosis was present in some areas.IMMUNOHISTOCHEMISTRY AND FLOW CYTOMETRY
A. Lymph node:
Immunohistochemistry: Blastic cells were positive for CD1a, CD2, CD3, CD4, CD5, CD7, TdT, and Ki67 (almost 100% labeling index). Blastic cells were negative for B-cell markers. A few cells were positive for CD117, CD15, CD33, myeloperoxidase, and lysozyme.Flow cytometric analysis: Blast cells were positive for CD45 (intermediate intensity), CD1a, CD2, cytoplasmic CD3, CD4, CD5, CD7, CD56 (dim), CD99, and TdT. There was loss of surface CD3. B-cell markers were negative. Myeloid markers were not used in the panel.B. First Bone Marrow:Immunohistochemistry: Rare CD34+ blasts, a few myeloperoxidase+ cells, a few small CD20+ cells, a few small CD3+ cells, no TdT+ cells, and many CD61+/Fctor VIII-related antigen+ megakaryocytes.C. Second Bone Marrow:Immunohistochemistry: Numerous CD34+ blasts, no CD3+ blasts, a few CD117+/myeloperoxidase+ cells, no TdT+ cells.Flow Cytometric Analysis: Myeloblasts accounted for approximately 80% of all cells analyzed and demonstrated posivity for: CD45, CD34, CD33, CD13, HLA-DR, CD11b,myeloperoxidase, CD15, CD4, CD5 (dim), CD7 (dim), and My4 (dim). Blasts did not express CD1a, CD2, CD3, CD8, CD19, CD20, CD10, CD56, CD117, CD16, CD64, Mo2, or TdT.CYTOGENETIC FINDINGS
C. Second Bone marrow: t(8;13) was detected.
Cell Line #1: 50,XX,+8,t(8;13)(p12;q12),+13,+13,der(13)t(8;13)x2,+21 Cell Line #2: 51,XX,+8,t(8;13)(p12;q12)x2,+13,+13,der(13)t(8;13)x2,+21,+marMOLECULAR FINDINGS
A. Lymph node: Interphase FISH demonstrated an FGFR1 rearrangement in 46% cells examined by using a breakapart probe.
C. Second bone marrow: Interphase and metaphase FISH on bone marrow aspirate for FGFR1 Involvement in t(8;13) was positive. nuc ish 8p12(FGFR1x2)(3`FGFR1 sep 5`FDGFR1x1)[17]/8p12(3`FGFR1x4,5`FGFR1x3)(3`FGFR1 con 5`FGFR1x1)[34]/8p12(3`FGFR1x4,5`FGFR1x2)(3`FGFR1 con 5`FGFR1x1)[80]/8p12(3`FGFR1x5,5`FGFR1x2)(3`FGFR1x2)[53]INTERESTING FEATURES
1. We predicted t(8;13) when we diagnosed T-lymphoblastic lymphoma with a minor myeloid component in a lymph node (bilineal myeloid/T-lymphoid lymphoma) and also found absolute eosinophilia in the blood and a myeloproliferative neoplasm with richness of eosinophils and eosinophil precursors in the bone marrow. About 6 months later she developed acute myeloid leukemia (AML) with t(8;13)(p12;q12). After the diagnosis of AML, we did FISH for FGFR1 abnormality on the lymph node with bilineal lymphoma and found FGFR1 rearrangement. Bilineal lymphomas have been described in 8p11 myeloproliferative syndrome (EMS), which should now be called 8p12 myeloproliferative syndrome [1]
Please note that the location of FGFR1 gene has been changed to 8p12 from 8p11.2 recently. 2. Our case had absolute basophilia in addition to absolute eosinophilia when she presented with T-LBL with minor myeloid component. Absolute basophilia is usually found in patients with t(8;22)(p11;q11). We did not have t(8;22)(p11;q11), but had t(8;13)(p12;q12) [2].3. In addition, we found trisomy 8 and trisomy 21 in the bone marrow with AML. These findings are common in AML that develops in a patient with MPN with EMS [2,3].4. We detected FGFR1 rearrangement both in the lymph node with bilineal lymphoma and in the bone marrow with AML. This finding has been reported in the literature [2]. The lymph node had a minor myeloid component, but the detection of FGFR1 rearrangement in 46% cells indicates presence of FGR1 abnormality also in the lymphoblasts.5. First bone marrow biopsy after the diagnosis of bilineal lymphoma showed marked fibrosis in a large area of the biopsy. This degree of fibrosis of bone marrow is an interesting finding in EMS.References:1. Vega F, Medeiros LJ, Davuluri R, Cromwell CC, Alkan S, Abruzzo LV. t(8;13)-bilineal lymphomas: report of 6 cases. Am J Surg Pathol 2008;32:14-20.2. Jackson CC, Medeiros JL and Miranda RN. 8p11 myeloproliferative syndrome: a review. Hum Pathol 2010;41:461-476.3. Agerstam H, Lilljebjorn H, Lassen C, Swedin A, Richter J, Vandenberghe P, Johnaason B, Fioretos T. Fusion-gene mediated truncation of RUNX1 as a potential mechanism underlying disease progression in the 8p11 myeloproliferative syndrome. Genes Chromosomes Cancer 2007;46:635-643.PROPOSED DIAGNOSIS
T-lymphoblastic lymphoma (T-LBL) with a minor component of immature and mature myeloid cells (bilneal myeloid/T-lymphoid lymphoma), myeloproliferative neoplasm followed by acute myeloid leukemia (AML) with FGFR1 rearrangement in the lymph node as well as in the bone marrow with AML (WHO Classification: Myeloid and lymphoid neoplasm with FGFR1 abnormality)
CONSENSUS DIAGNOSIS
Myeloid and lymphoid neoplasm with FGFR1 rearrangement, t(8;13)(p12;q12), presenting with T-lymphoblastic lymphoma and myeloproliferative neoplasm, followed by acute myeloid leukemia
| Touch imprint showing numerous blasts and a few eosinophils/eosinophil precursors (DiffQuik Stain) |  |
| Lymph node with sheets of blasts |  |
| Lymph node showing sheets of blasts and a few eosinophils/eosinophil precursors |  |
| Immunostain for CD1a shows positivity in the blasts |  |
| Immunostain for CD3 shows positivity in the blasts |  |
| Immunostain for CD117 shows a few positive cells. | 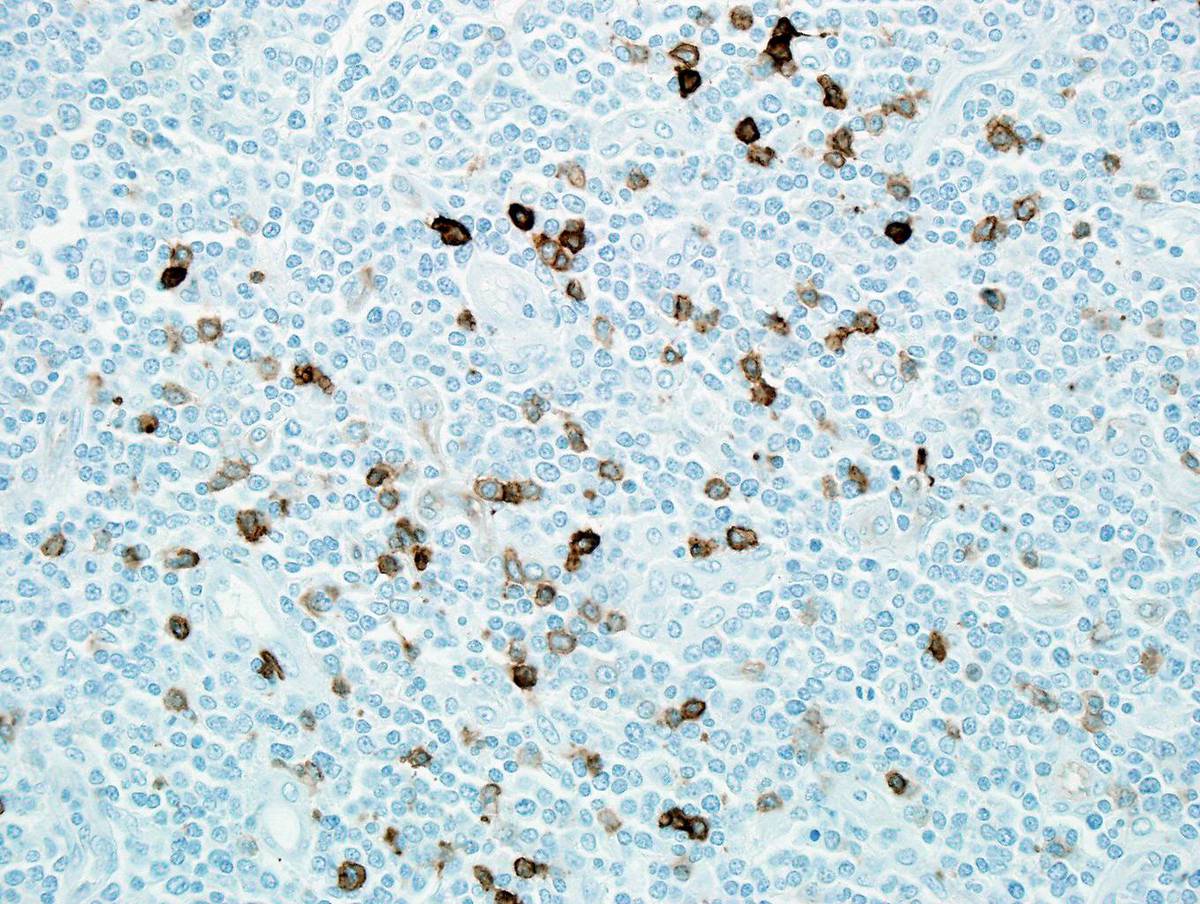 |
| Immunostain for CD33 shows a few positive cells. |  |
| Immunostain for myeloperoxidase shows a few positive cells. |  |
| Immunostain for TdT is positive in the blasts in the lymph node. | 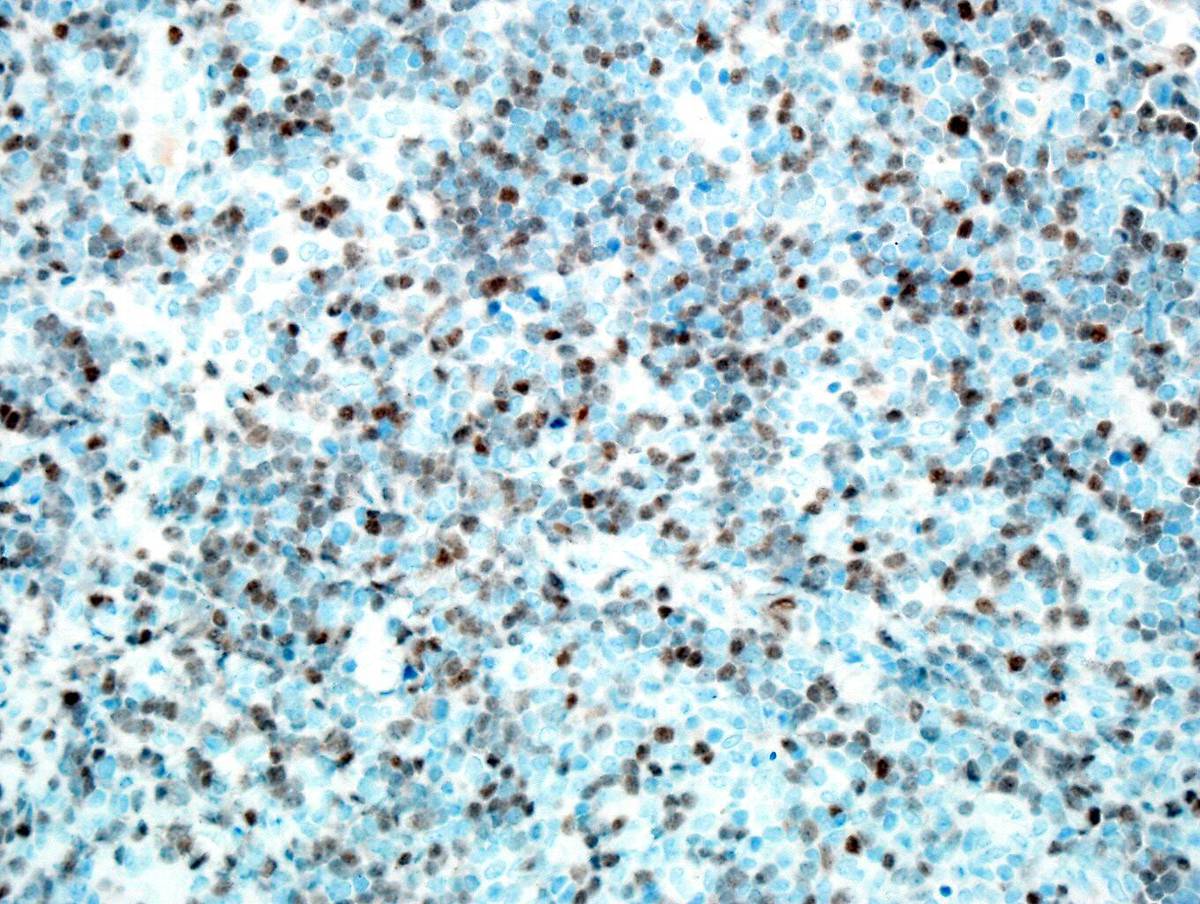 |
| Immunostain for Ki67 shows Ki67 positivity in almost 100% cells. | 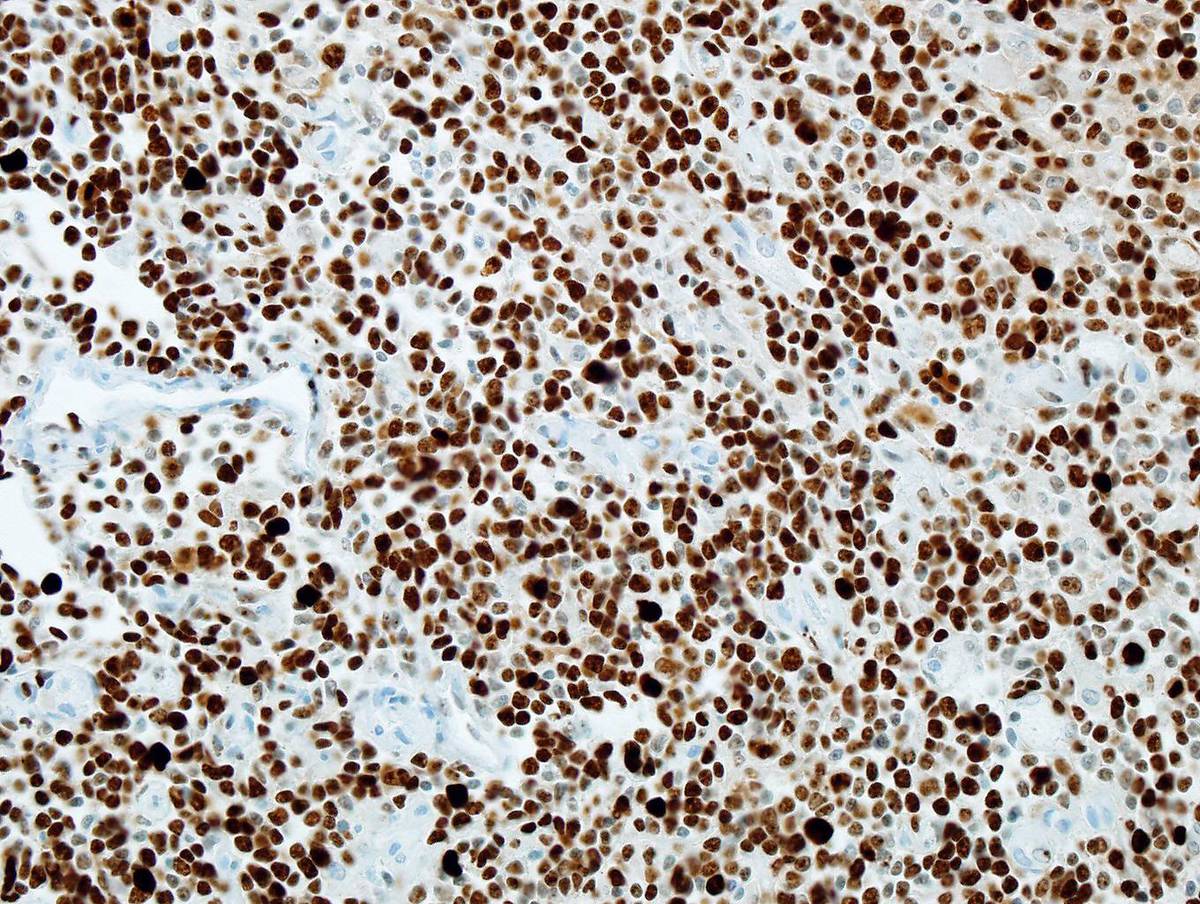 |
| Bone marrow core biopsy shows sheets of eosinophils and eosinophil precursors. |  |
| Bone marrow core biopsy with areas of marked fibrosis. |  |
| Reticulin stain shows marked reticulin fibrosis. | 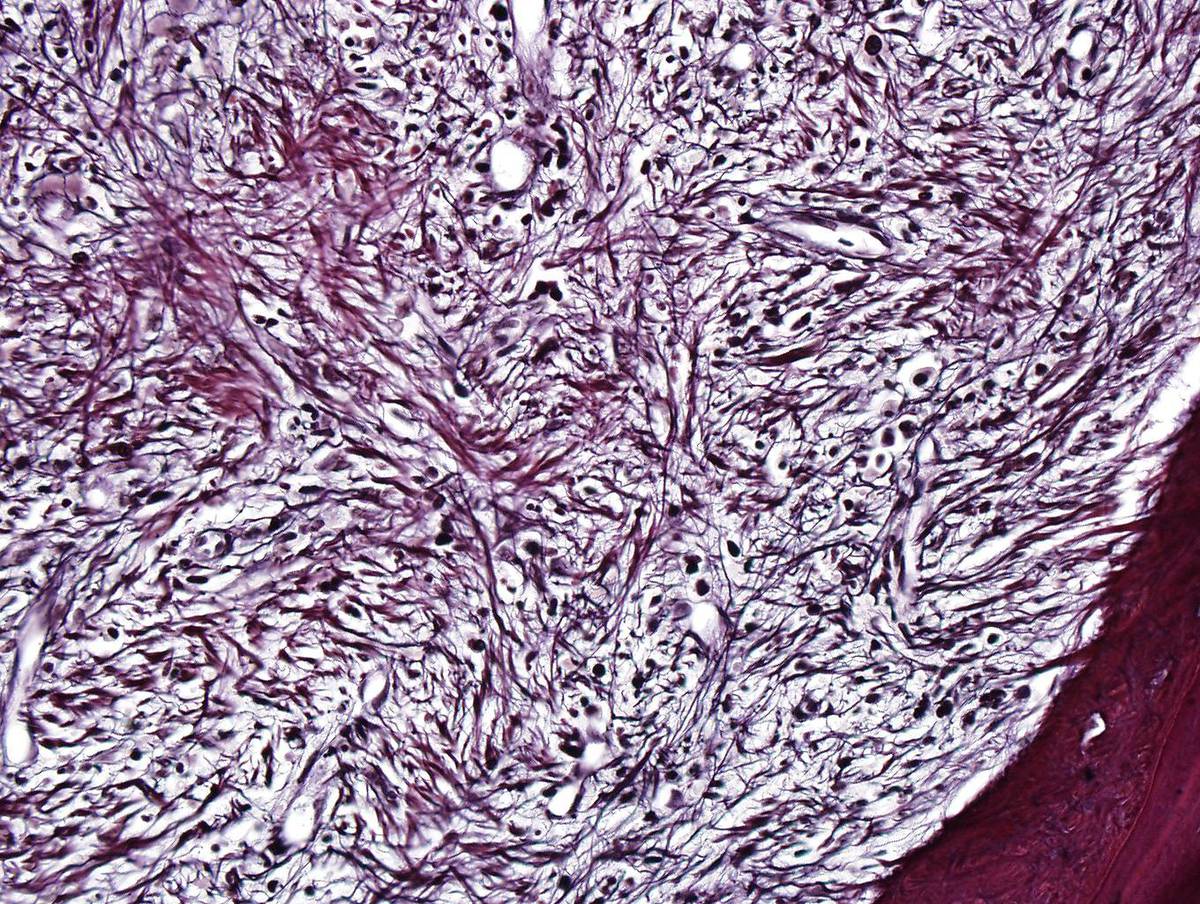 |
| Immunostain for CD61 on the bone marrow core shows increased megakaryocytes. |  |
| Second bone marrow aspirate shows numerous blasts. | 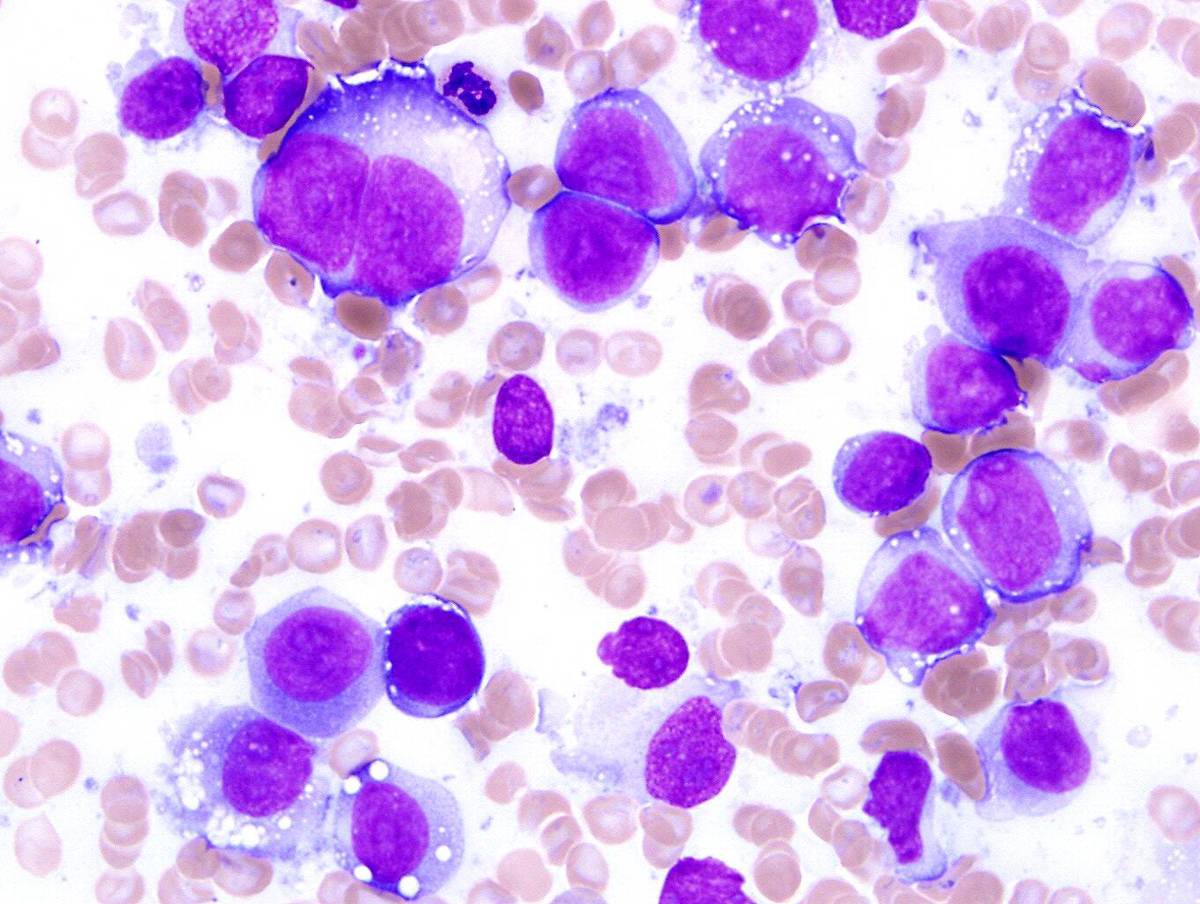 |
| Second bone marrow core shows sheets of blasts. |  |
| Second bone marrow core shows fibrosis. | 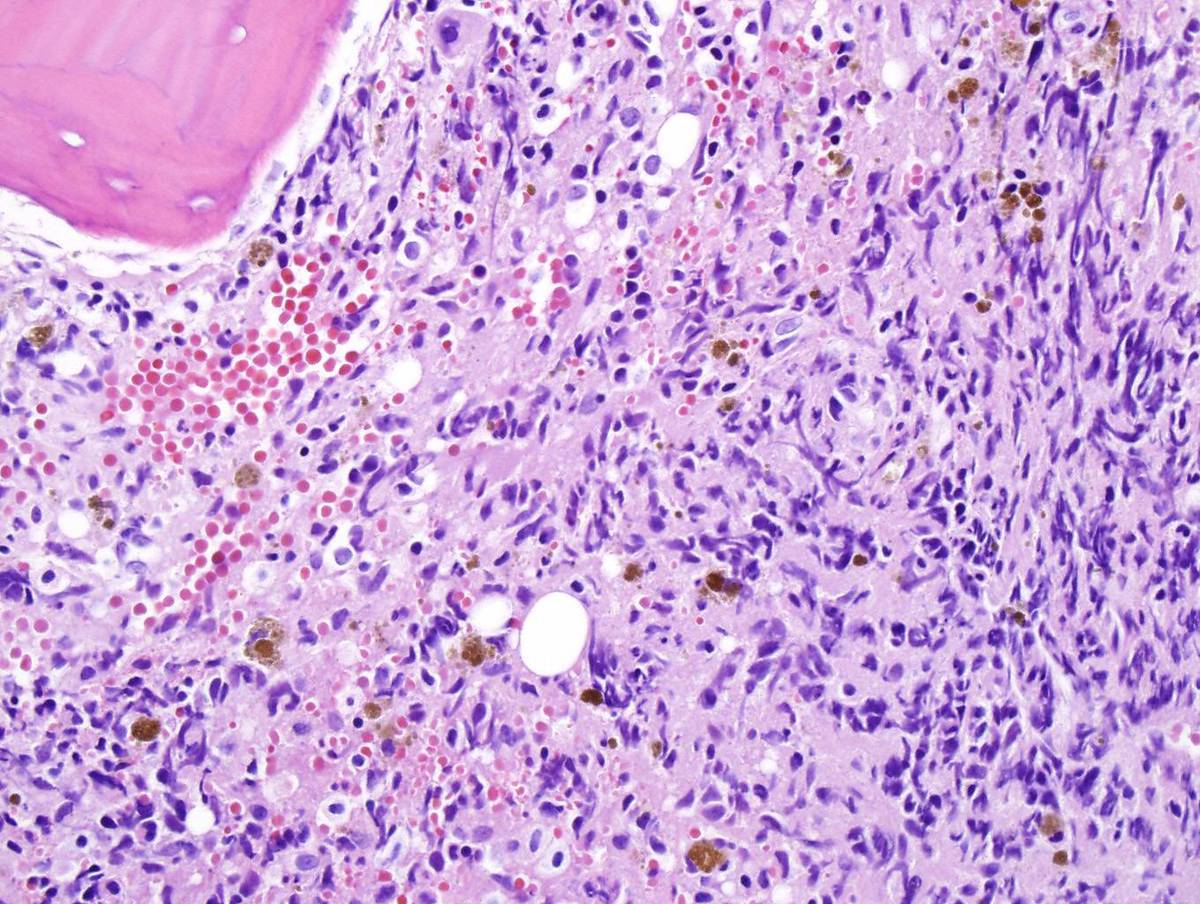 |
| Second bone marrow core shows strong and diffuse CD34 positivity. |  |
| Cytogenetic analysis of second bone marrow shows t(8;13). |  |
| Cytogenetic analysis of second bone marrow shows t(8;13) in second cell line. |  |
| Metaphase FISH in second marrow shows involvement of FGFR1 in t(8;13) in one cell line (breakapart probe) |  |
| Metaphase FISH in second marrow shows involvement of FGFR1 in t(8;13) in second cell line (breakapart probe) | 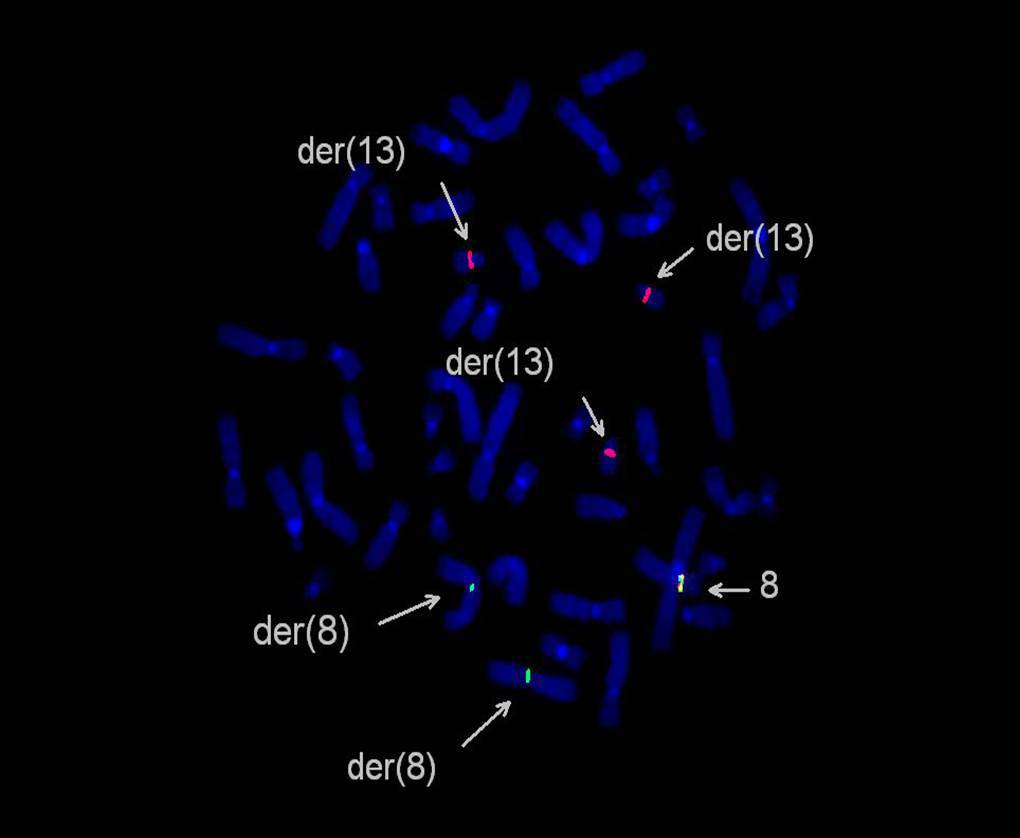 |
| Interphase FISH in second marrow shows involvement of FGFR1 in t(8;13) - breakapart probe was used. | 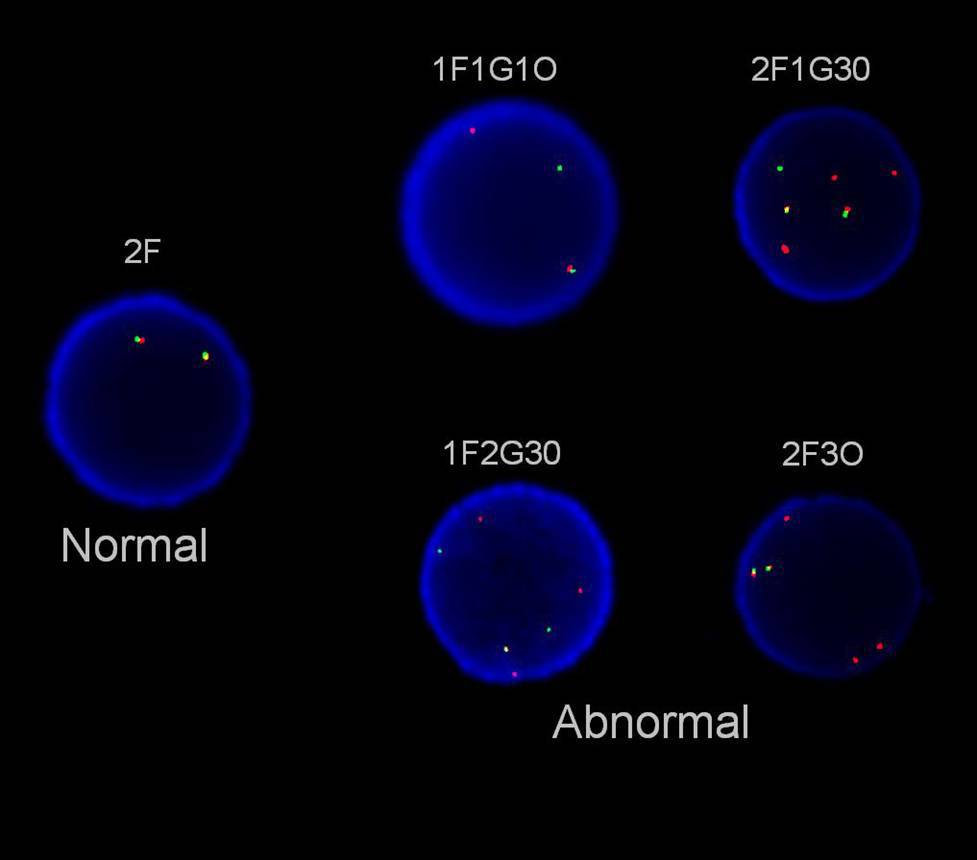 |
| Interphase FISH in lymph node with bilineal lymphoma shows FGFR1 rearrangement (breakapart probe). | 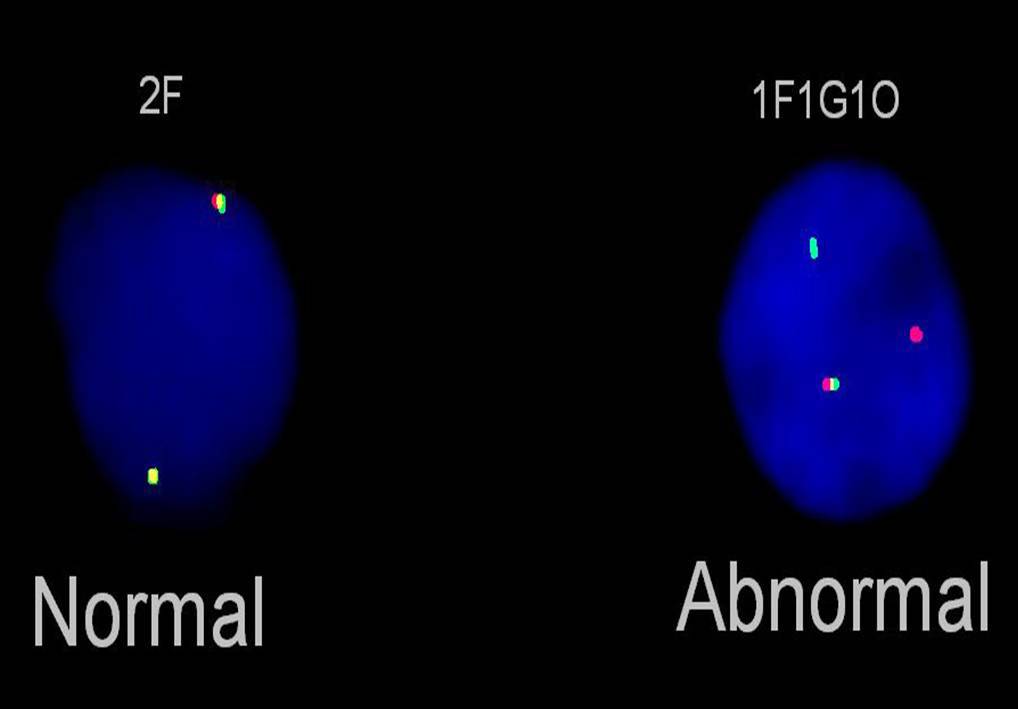 |