Institution: Genoptix Medical Laboratory
Additional authors:Hong Drum, Aine Yung, Bashar Dabbas
Session: Therapy-related myeloid neoplasms
HISTORY
A 56-year-old female with a history of diffuse large B-cell lymphoma, status post chemotherapy 3 years prior, presented with new onset of leukocytosis (WBC 47 K/uL) and thrombocytopenia (PLT 68 K/uL). A bone marrow biopsy with aspiration was performed to rule out recurrent lymphoma.
DETAILS
Sections of the core biopsy (iliac crest processed with B+ fixative and decalcified) showed a hypercellular bone marrow diffusely replaced by blasts (Figure 1). Aspirate smear revealed the majority of the blasts to be of intermediate to large size with oval nuclei, prominent nucleoli, and variable amounts of agranular cytoplasm containing vacuoles (Figure 2). Erythrophagocytosis was identified (Figure 3). Normal trilineage hematopoiesis was markedly decreased. There was no morphologic evidence of lymphoma. Concurrent peripheral blood smear showed marked leukocytosis with increased blasts (50%). Many of the blasts in the peripheral blood displayed more folded nuclei and more abundant cytoplasm than those in the bone marrow (Figure 4). Thrombocytopenia was also present.
IMMUNOHISTOCHEMISTRY AND FLOW CYTOMETRY
Flow cytometry showed an expanded myelomonocytic population (70%) with intermediate to high side scatter, positive for CD11b (variable), CD13 (variable), CD33, HLA-DR (bright), CD45 (moderate), and CD4, and negative for CD34, CD117, and CD7. A monoclonal B-cell population was not detected. Immunostain for MPO was positive in the blasts (Figure 5).
CYTOGENETIC FINDINGS
Karyotype showed 46,XX,t(8;16)(p11.2;p13.3)[19]/46,XX[1] (Figure 6).
MOLECULAR FINDINGS
Molecular analysis was negative for FLT3-ITD, FLT3-D835, and NPM1 mutations.
INTERESTING FEATURES
In the current WHO classification, acute myeloid leukemia (AML) with t(8;16) is not included in the category of AML with recurrent genetic abnormalities or described under therapy-related myeloid neoplasms. However, while rare, it is clear from the literature that AML with t(8;16) displays distinct clinicopathologic features. The submitted case demonstrates several of these features, including a history of chemotherapy for a prior malignancy, monocytic differentiation by morphology and flow cytometry, and erythrophagocytosis. Additional features characteristic of this entity but unknown in this case include increased risk of disseminated intravascular coagulation, extramedullary involvement, and poor prognosis.
PROPOSED DIAGNOSIS
Therapy-related AML with t(8;16).
CONSENSUS GROUP: ADDITIONAL INFORMATION/STUDIES
Additional immunostains performed by the conference consensus group:
PGM1: Negative
CONSENSUS DIAGNOSIS
Therapy-related myeloid neoplasm, acute myeloid leukemia with t(8;16)(p11.2;p13.3)
| Figure 1: Hypercellular bone marrow diffusely replaced by blasts |  |
| Figure 2: Intermediate to large blasts with oval nuclei, prominent nucleoli, and variable amounts of agranular cytoplasm containing vacuoles |  |
| Figure 3: Erythrophagocytosis | 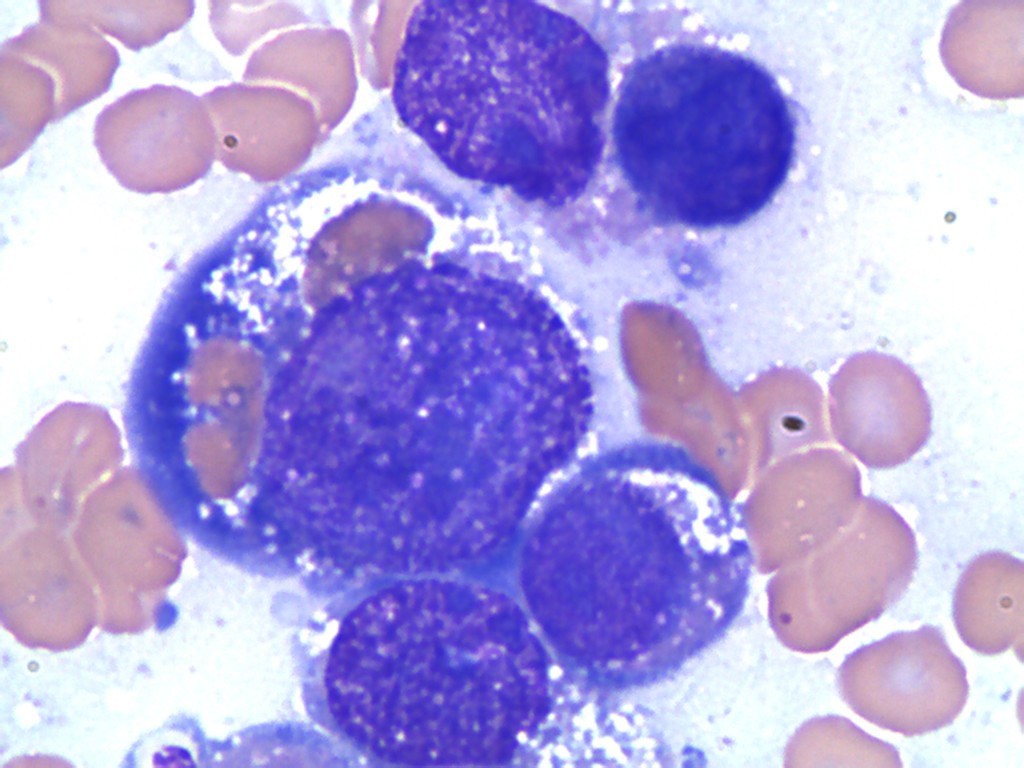 |
| Figure 4: Peripheral blood blasts displaying more folded nuclei and more abundant cytoplasm than those in the bone marrow |  |
| Figure 5: MPO positive in blasts |  |
| Figure 6: 46,XX,t(8;16)(p11.2;p13.3)[19]/46,XX[1] | ![Figure 6: 46,XX,t(8;16)(p11.2;p13.3)[19]/46,XX[1]](cases/222/images/Figure 61.jpg) |