Institution: The University of Texas Southwestern Medical Center
Additional authors:Imran Shahab, Prasad Koduru, Hung Luu
Session: Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB, or FGFR1
HISTORY
A 44 year-old male rancher noted upper back pain for about one month. An MRI of the cervical and thoracic spine revealed a soft tissue paraspinal mass extending from C7 to T2 (image 1). He underwent open biopsy of the mass, posterior T1 and T2 laminectomy, and decompression of the tumor circumferentially from around the spinal cord. A bone marrow biopsy was performed four days later and the CBC and differential revealed: WBC 7.6 x 109/L, HGB 12.1 g/dL, MCV 97 fL, RDW 13.2%, PLT 243 x 109/L; Neutrophils 3.6 x 109/L, Lymphocytes 0.91 x 109/L, Monocytes 0.23 x 109/L, Eosinophils 2.7 x 109/L, and Basophils 0.08 x 109/L.
DETAILS
The biopsy of the paraspinal mass revealed sheets of medium-sized to large, immature-appearing cells with round to indented nuclei and a moderate amount of cytoplasm (images 2). The immature-appearing cells included a substantial proportion of eosinophil precursors (image 3) and Charcot-Leyden crystals were present (black arrows, image 4). The peripheral blood film revealed an absolute eosinophilia comprised of mature forms with occasional cytoplasmic clearing, but without overt abnormalities (image 11). The bone marrow aspirate smear was paucispicular, but revealed an increased proportion of eosinophils without an increase in blasts (image 12). The bone marrow biopsy was hypercellular (80%) with slightly increased megakaryocytes (including a few hyperchromatic forms), increased granulocytic precursors (including increased eosinophil precursors) and adequate erythroid precursors with progressive maturation (image 13-15). The bone marrow biopsy also displayed loose collections of mast cells, sometimes admixed with small lymphocytes, which were better appreciated on immunohistochemistry.
IMMUNOHISTOCHEMISTRY AND FLOW CYTOMETRY
Immunostains done on the paraspinal mass showed the that the majority of cells were negative for CD34 (image 5), only a few cells positive for CD117 (image 6), a subset positive for myeloperoxidase (image 7), a subset positive for CD68 PG-M1 (image 8) , and a subset positive for lysozyme (image 9). Immunostains done on the bone marrow biopsy showed no increase in CD34 positive blasts. Most cells were negative for CD117, but focal collections of mast cells were positive (image 16). Tryptase was also positive in the mast cells. Flow cytometry was not done on the mass and did not reveal any abnormalities for the marrow.
CYTOGENETIC FINDINGS
Cytogenetic FISH analysis performed on paraffin embedded sections from the paraspinal mass was positive for deletion of the CHIC2 gene, indicating fusion of FIP1L1/PDGFRA (image 10); a normal pattern has all three colors FIP1L1 (green probe), CHIC2 (red probe) and PDGFRA (blue probe) while CHIC2 deletion is indicated by a missing red signal (indicated by yellow arrows). Classical cytogenetic study of the bone marrow aspirate revealed a normal male karyotype; FISH analysis on the bone marrow aspirate was positive for deletion of the CHIC2 gene in 28.5% of 200 interphase nuclei and was negative for BCR/ABL1, PDGFRB rearrangement, FGFR1 rearrangement, RUNX1T1/RUNX1, MLL rearrangement and CBFB rearrangement.
MOLECULAR FINDINGS
Not done.
INTERESTING FEATURES
Myeloid and lymphoid neoplasms with FIP1L1-PDGFRA are rare, have a striking male predominance, and are very sensitive to low-dose imatinib. The disease features most commonly resemble chronic eosinophilic leukemia. The disease also rarely presents with concomitant acute myeloid leukemia (AML), including myeloid sarcoma (MS), and/or with concomitant T lymphoblastic lymphoma (T-LL). In general, MS behaves similar to AML and requires aggressive therapy. However, there are increasing reports of patients with FIP1L1-PDGFRA-associated disease that present with phenotypically aggressive features (i.e. AML, MS or T-LL) who have achieved complete remission and durable disease-free survival with imatinib alone. Rare patients develop imatinib resistant mutations (PDGFRA T6741 and D842V mutations) with features of an accelerated phase or blast transformation. Imatinib-resistant disease may respond to second generation tyrosine kinase inhibitors, but consideration for allogeneic stem cell transplant may be recommended at this point since response could be short lived. The presented patient received induction chemotherapy using cytarabine and idarubicin. Day 14 marrow was markedly hypocellular and cytogenetics/FISH was normal without evidence for FIP1L1/PDGFRA. Day 28 marrow was normocellular without eosinophilia ; cytogenetics revealed a normal karyotype, but FIP1L1/PDGFRA rearrangement was detected by FISH in 2.5% of 200 interphase nuclei. An MRI showed resolution of the paraspinal mass. The patient was then started on imatinib and has also completed three cycles of consolidation using high dose cytarabine. After consolidation, he will receive imatinib maintenance. In the event of a relapse, there is also a search for an allogeneic donor.
PROPOSED DIAGNOSIS
Myeloid neoplasm with FIP1L1-PDGFRA presenting as a myeloid sarcoma and a myeloproliferative neoplasm with eosinophilia.
CONSENSUS DIAGNOSIS
Myeloid neoplasm with FIP1L1-PDGFRA rearrangement, presenting as myeloid sarcoma and myeloproliferative neoplasm with eosinophilia
| Image 1, MRI of cervical & thoracic spine |  |
| Image 2, paraspinal mass (H&E) |  |
| Image 3, paraspinal mass (H&E) |  |
| Image 4, paraspinal mass with Charcot-Leyden crystals (arrows) | 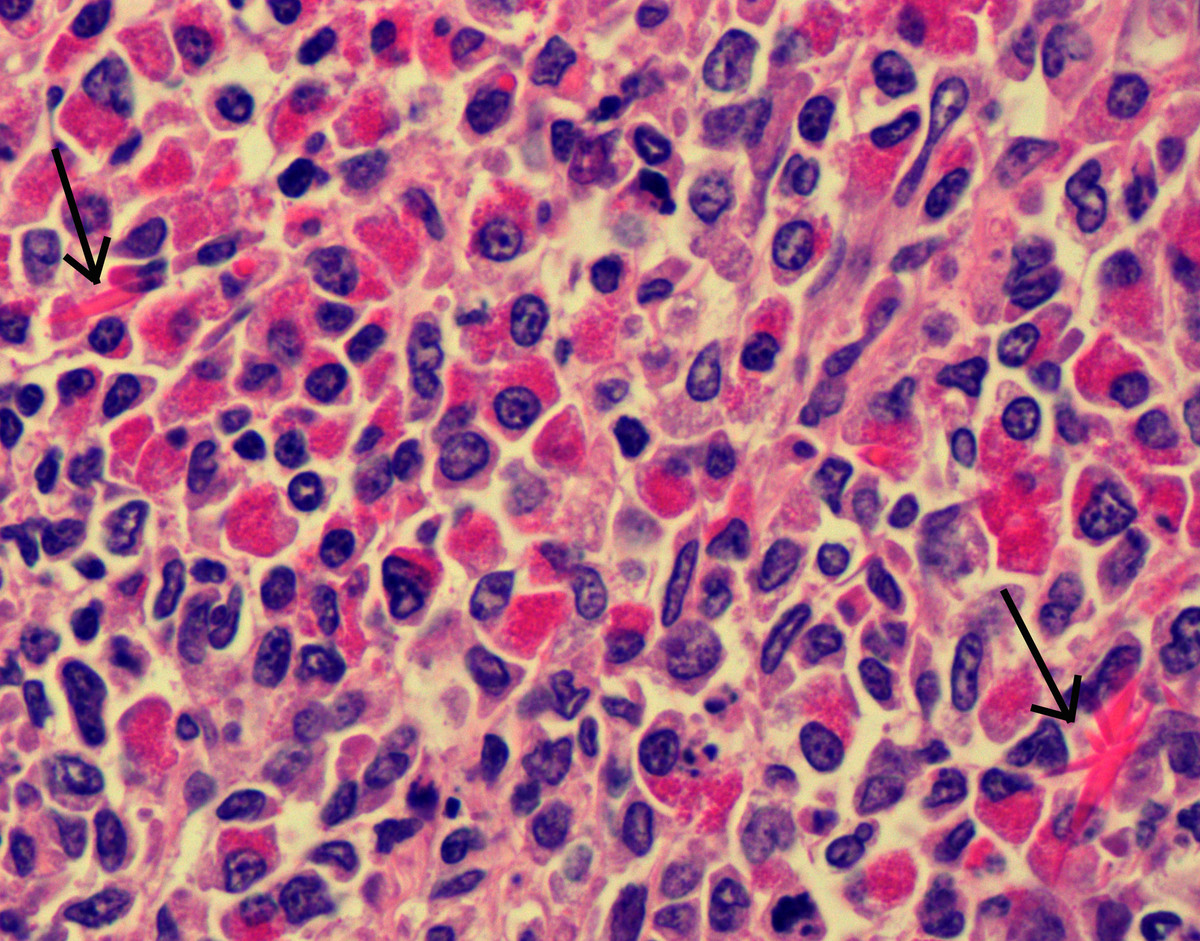 |
| Image 5, CD34 on paraspinal mass |  |
| Image 6, CD117 on paraspinal mass |  |
| Image 7, MPO on paraspinal mass |  |
| Image 8, CD68 PG-M1 on paraspinal mass |  |
| Image 9, lysozyme on paraspinal mass |  |
| Imag 10, FISH for CHIC2 deletion on paraspinal mass |  |
| Image 11, peripheral blood film |  |
| Image 12, aspirate smear |  |
| Image 13, bone marrow biopsy (low power) |  |
| Image 14, bone marrow biopsy (medium power) |  |
| Image 15, bone marrow biopsy (high power) |  |
| Image 16, CD117 on bone marrow biopsy | 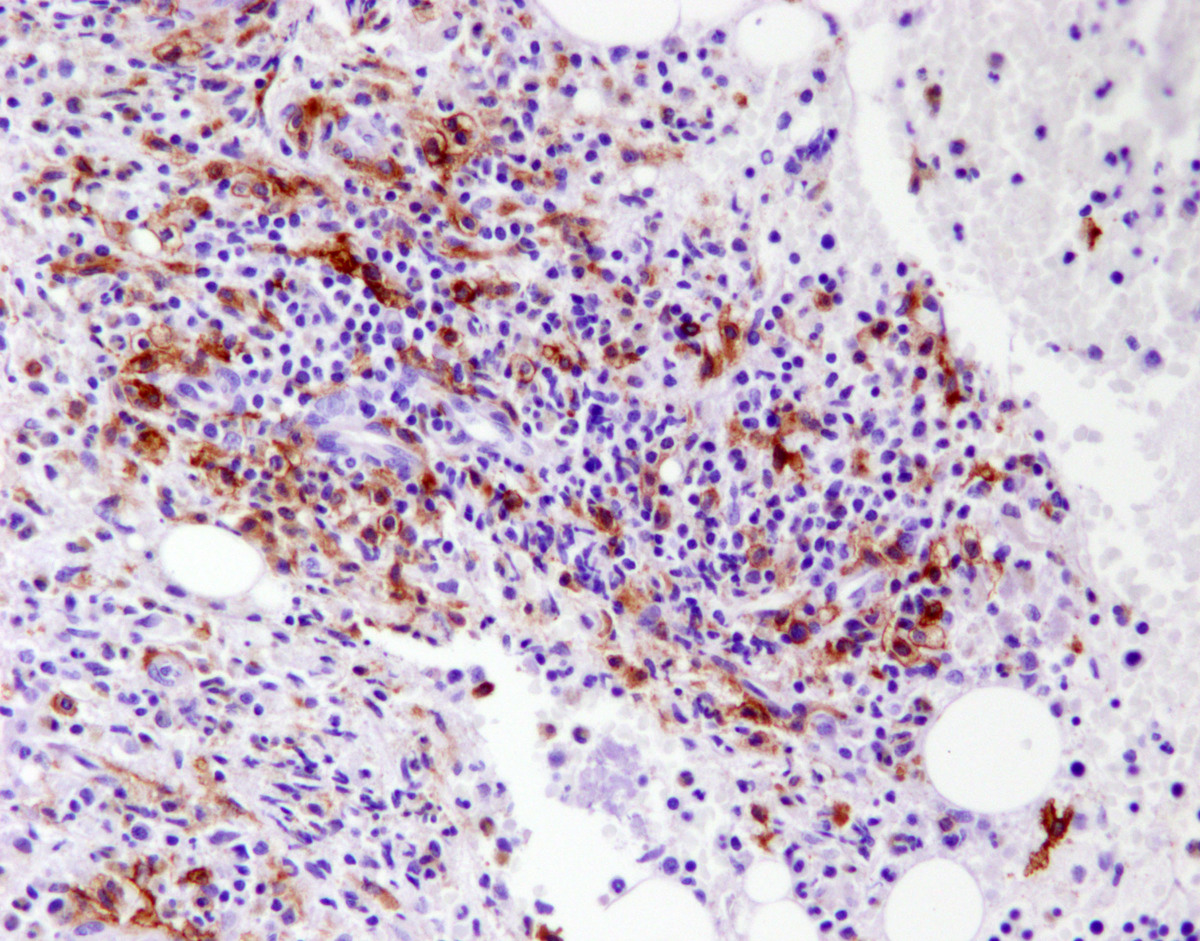 |