Institution: Wake Forest School of Medicine
Additional authors:David D. Grier, MD
Session: Therapy-related myeloid neoplasms
HISTORY
A 56-year old male with a history of non-small cell lung carcinoma status post chemotherapy and radiation, presented approximately two years later with non-exertional chest pain. CT scan revealed adenopathy in multiple sites and splenomegaly. Leukocytosis, anemia and thrombocytopenia were observed on CBC, with greater than 50% blasts. The bone marrow was involved by T lymphoblastic leukemia. The patient completed chemotherapy successfully. Fifteen months after the initial diagnosis the patient was admitted for pneumonia and was found to be pancytopenic. A bone marrow biopsy revealed increased blasts.
DETAILS
Both diagnoses were obtained through bone marrow biopsies, which were fixed in B+. Microscopically, the T-cell lymphoblasts were variable in size, with prominent nucleoli and scant basophilic cytoplasm with no vacuoles. The bone marrow involved by AML was 80-90% cellular with 23% blasts. The blasts had irregular nuclear outlines and abundant vacuolated cytoplasm. Increased monocytic fraction of 68% was noted. No Auer rods were seen.
IMMUNOHISTOCHEMISTRY AND FLOW CYTOMETRY
By flow cytometry, the T lymphoblasts expressed CD34, CD10 (dimly), and cytoplasmic CD3 without surface CD3 expression. The blasts did not express CD19, cytoplasmic myeloperoxidase (MPO), or nTdT. Immunohistochemistry revealed that the cells were reactive with antibodies to CD34, CD10, and CD79a. They are negative for CD117 and MPO. The myeloid blasts expressed MPO and muramidase and were negative for CD34, CD117, CD10, TdT, CD3, CD19 and CD79a by immunohistochemistry. Flow cytometry reveals increase in blast population (35%) that expresses CD33, CD38, HLA-DR (dim), MPO, CD36, CD64, CD11b and CD56 (subset) without expression of CD34, CD117, CD10, nTdT, CD19, CD20 and cytoplasmic CD3. No increase in T-lymphoblasts or atypical T-cell population was identified.
CYTOGENETIC FINDINGS
T lymphoblasts: 50,XY,+13,+13,+20,+21 Myeloid blasts: 46,XY,t(4;11)(q21;p15),add(12)(p13)
MOLECULAR FINDINGS
INTERESTING FEATURES
t(4;11) is most commonly found in B lymphoblastic leukemia, and is exceptionally rare in T lymphoblastic leukemia. Interestingly, it was this patient’s AML that had this translocation and not the T lymphoblastic leukemia. The AML appears to be a completely different clonal process that most likely developed secondary to the patient’s lung cancer therapy.
PROPOSED DIAGNOSIS
Therapy related acute myeloid leukemia
CONSENSUS DIAGNOSIS
Therapy-related myeloid neoplasm; acute myeloid leukemia
| AML core biopsy | 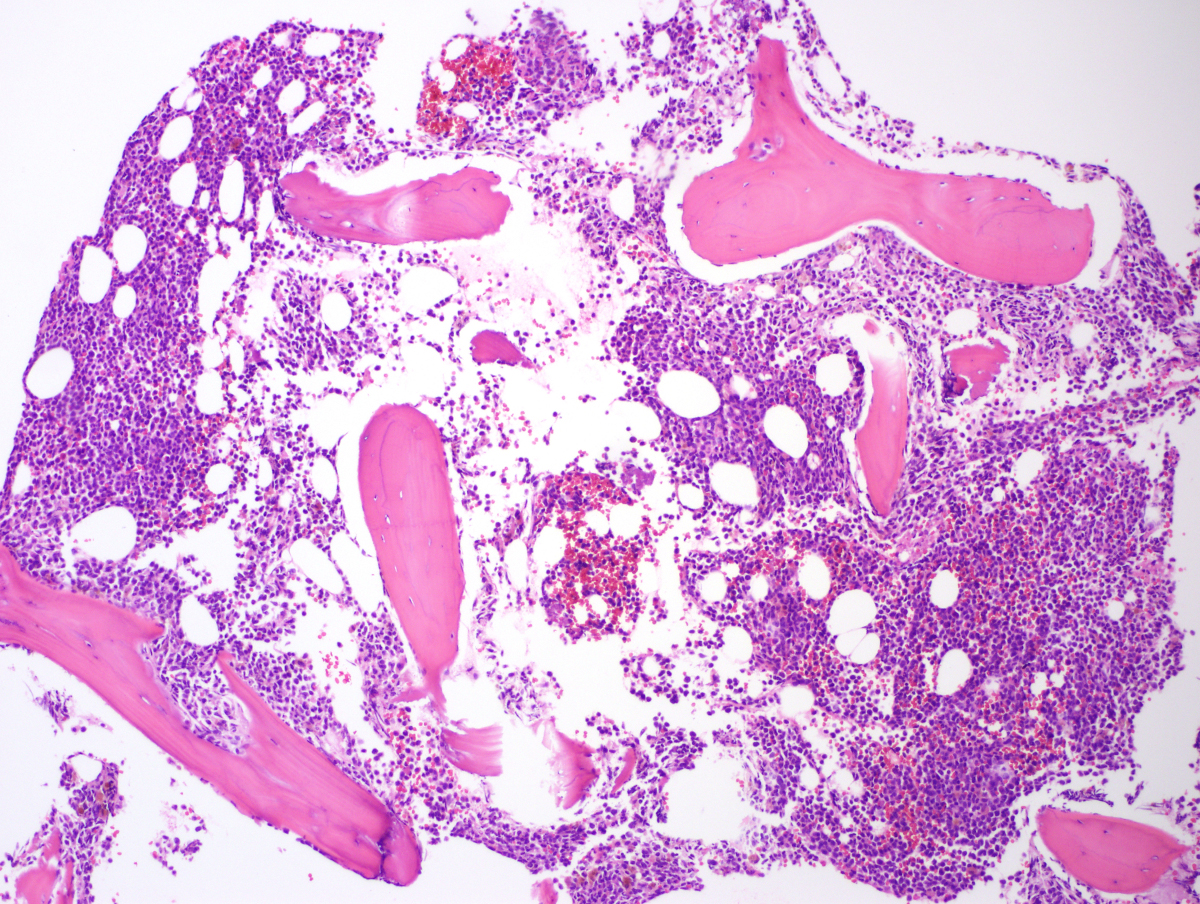 |
| AML core biopsy 600x |  |
| AML aspirate smear |  |
| AML core biopsy CD3 | 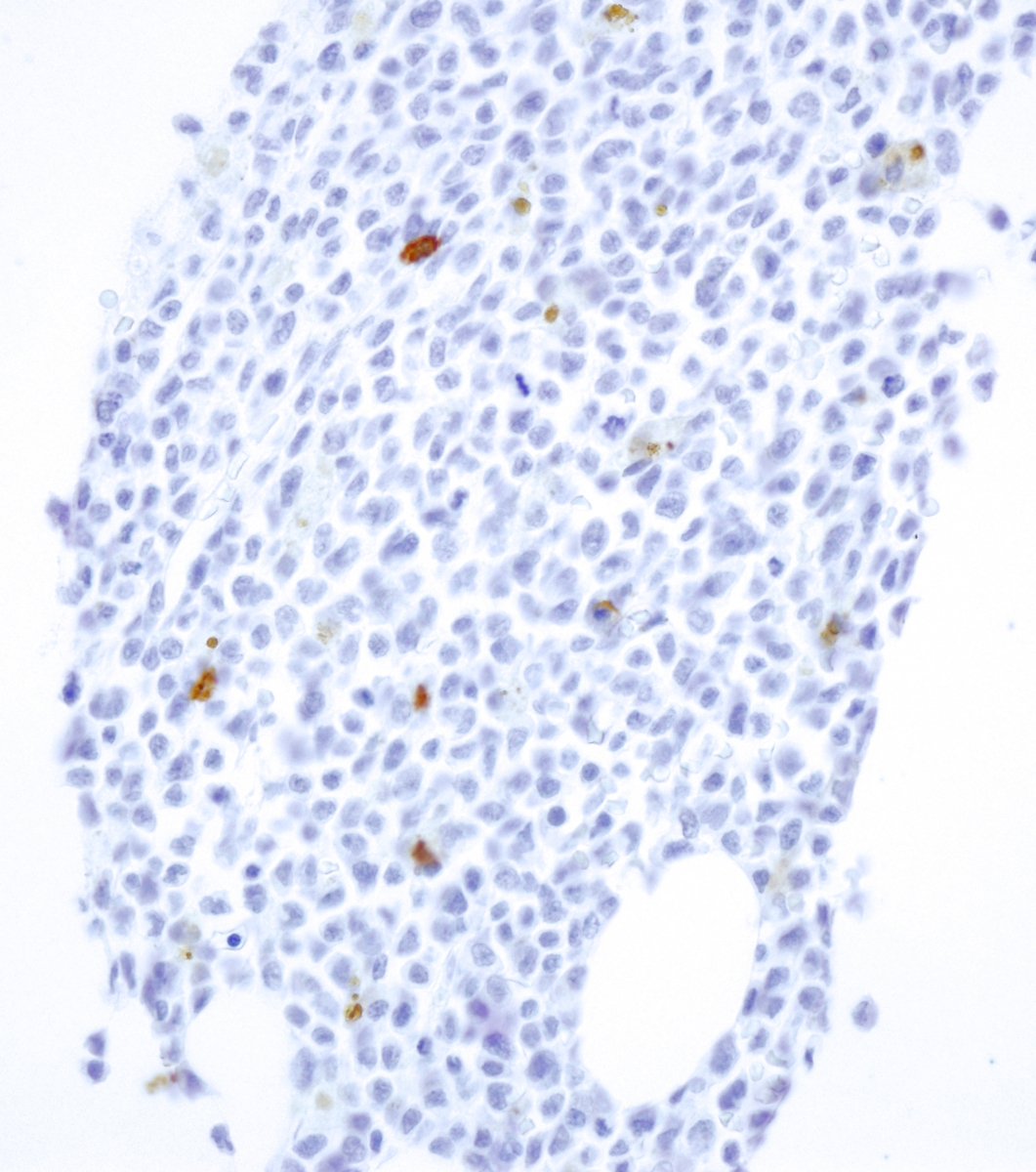 |
| AML core biopsy myeloperoxidase |  |
| AML core biopsy muramidase |  |
| T-ALL core biopsy |  |
| T-ALL core biopsy 600x |  |
| T-All smear |  |