Institution: Roswell Park Cancer Institute
Additional authors:Vishala Neppalli MD, Sheila N. Jani Sait PhD, Francisco Hernandez-Ilizaliturri MD
Session: Acute leukemias of ambiguous lineage
HISTORY
The patient is a 63 year-old male who is status post chemotherapy with R-CHOP for nodal follicular lymphoma (grade 3B, 15%) and diffuse large B-cell lymphoma. Staging bone marrow was negative for a lymphoproliferative neoplasm and acute leukemia by morphology, flow cytometry and molecular studies (polyclonal B cell gene rearrangement and negative BCL2 translocation), Peripheral blood indices at diagnosis showed only mild normocytic anemia of 12.4 g/dL. Seven months post chemotherapy, the patient presented with marked leukocytosis (WBC 493.98 x10^9/L). The bone marrow and peripheral blood showed B lymphoblastic leukemia (BLL) and hyper-CVAD module A chemotherapy was initiated. Cycle 1 was administered and complicated with pulmonary distress and intracranial hemorrhage. The patient was put on Neupogen (Filgrastim) for low absolute neutrophil count. Total of 6 cycles were delivered, thereafter the patient had relapsed acute leukemia and re-induction with clofarabine ended with refractory disease. During the clinical course of the patient’s disease, five bone marrow samples were obtained (staging for lymphoma, BM-L, diagnostic for BLL, BM-1, before initiation cycle 2, BM-2, before initiating cycle 5, BM-3, and after re-induction, BM-4).
DETAILS
All evaluated bone marrow and blood smears were Wright-Giemsa stained.
BM-1 sample: The blood and the bone marrow smears had dominant population of blasts (90%) with variable morphology including large sized, irregularly nucleated (with occasional cup-shaped), and occasional vacuolated forms but without definite Auer rods. BM-2 sample: The blood had pancytopenia with monocytosis (mainly mature) and the bone marrow smears showed dominant population of monocytoid cells with dominant immature forms (77%). BM-3: The bone marrow had no definite morphologic evidence of acute leukemia (blasts 2%, dyshematopoiesis, and few monocytes); blood smear is not available for review. BM-4: The blood smear had marked leukopenia; the bone marrow smears showed relapsed acute leukemia with frequent blasts (40%) and monocytoid cells (35%).IMMUNOHISTOCHEMISTRY AND FLOW CYTOMETRY
All evaluated core biopsies are FFPE and decalcified.
BM-1 sample: The blasts had the following cytochemical (performed on aspirate smears)/immunohistochemical (performed on core biopsy sections) phenotype; negative for cytochemical myeloperoxidase, Sudan black, chloroacetate esterase, and alpha naphthyl butyrate esterase, and positive for TdT (strong intensity), PAX5 (variable intensity), and CD79a (small portion), and negative for CD10, CD34, CD117, CD22, CD68, lysozyme, and BCL6 immunostains. Also the blasts (about 95% of total analyzed cells) had the following flow cytometry immunophenotype; expressing CD45 (dim), HLA-DR, CD19 (bright), CD22 (heterogeneous), CD38 (bright), and CD34 (subset), and CD32 and CD71 (heterogeneous), and lacking CD5, CD10, CD11c, CD11b, CD13, CD33, CD20, CD23, CD52, CD80, and surface light chain immunoglobulin expression. BM-2: The bone marrow core biopsy showed sheets of monocytoid cells positive for CD68, lysozyme (diffuse, strong intensity), and CD163 (weaker than background macrophages), and are otherwise negative for TdT (very sparse scattered nuclei are highlighted), CD34, CD117, CD10, PAX5, CD45RA, CD123, and myeloperoxidase immunostains. Flow cytometry, performed on the marrow aspirate, showed a prominent monocytic populating (49% of total analyzed cells) expressing CD45, HLA-DR (heterogeneous), CD14 (heterogeneous), CD11c, CD11b, CD13 (heterogeneous), CD33, and CD52 and lacking CD34 and CD117 expression (CD15 and CD64 were not performed ), and no definite evidence of the previously detected neoplastic B lymphoblastic population.BM-3: No immunostains are performed on the core biopsy. Flow cytometry, performed on the marrow aspirate, showed findings consistent with minimal residual acute leukemia with B-lymphoblastic immunophenotype. BM-4: The bone marrow core biopsy had sheets of immature-appearing cells (blasts), most of which with monocytoid features based on H&E stained sections; based on immunoperoxidase stained sections; the blasts were positive for TdT and PAX5 (50% or more of cells, similar staining pattern), CD68 (40%), and lysozyme (80%), and negative for CD79a, CD20, CD22, CD10, CD34, CD117, myeloperoxidase (highlighting sparse myeloid cells), and MUM1. Flow cytometry, performed on the marrow aspirate, showed two abnormal populations. The first is small to medium in size based on forward scatter (constituting 50% 0f analyzed cells) and expressing CD45 (dim), HLA-DR, CD19, CD22 (heterogeneous), CD38, and CD34 (subset), and lacking CD5, CD10, CD11c, CD11b, CD13, CD33, CD20, CD23, CD52, CD80, and surface light chain immunoglobulin expression. The second is larger based on forward scatter (20-30% of analyzed cells) and expressing CD45 (dim to bright), CD14, HLA-DR, CD4 (heterogeneous), CD11c, CD11b, CD13 (heterogeneous), CD33, CD38, and CD52.CYTOGENETIC FINDINGS
Conventional cytogenetics (karyotyping) were done on BM-1 and BM-2 samples and showed 46,XY,t(4;11)(q21;q23)[16]/46,XY,t(4;11)(q21;q23),del(7)(q22q34)[4], and 46,XY,t(4;11)(q21;q23)[13]/46,XY[7], respectively. Fluorescence in situ hybridization (FISH) analyses were done on all samples using the Vysis LSI MLL dual color break apart rearrangement probe (Abbott Molecular, Inc.). Split signals indicating an MLL rearrangement were seen and reported as the percentage of positive cells out of 200 interphase nuclei; 96% in BM-1, 73% in BM-2, 3% in BM-3, and 93% in BM-4.
FISHMOLECULAR FINDINGS
BM-1: Molecular analyses for FLT3 and NPM1 gene mutations showed FLT3-D835 mutation without definite evidence of ITD mutation, and wild-type NPM1 gene.
BM-1 to BM-4: Molecular analyses for B-cell IGH gene rearrangements (FR1-3) were monoclonal in all samples analyzed.INTERESTING FEATURES
This case harbors diagnostic and management challenges by presenting as pure B-lineage acute leukemia and switching to monocytic lineage post 1 cycle of Hyper-CVAD and adjuvant G-CSF therapy. Acute leukemia lineage, myeloid vs. lymphoid, is still the major determinant of the type of induction chemotherapy and the major question introduced by this case is: should this type of cases have separate line of management regardless of the lineage based on the detected translocation? In addition, the more important question at this time that may change the classification and probably the way the management planned is the designation of this acute leukemia as therapy-related as only 7 months lapsed since the completion of R-CHOP witch is short time for such definite determination. Regardless, it appears that at least the cytotoxic chemotherapy (R-CHOP) had in somehow role in accelerating what is genetically aberrant in this patients (germline or acquired). In this regard, molecular cytogenetic studies will be attempted on the lymphoma staging bone marrow sample, if available, to test for predisposing cryptic/minimal genetic abnormalities in this patient. It is still very critical and challenging to identify this group of patient who are at high risk of developing therapy-accelerated/therapy-related secondary hematopoietic malignancies upfront.
PROPOSED DIAGNOSIS
Possibly therapy-related/therapy-accelerated, acute leukemia of ambiguous lineage, mixed-phenotype acute leukemia with t(4;11)(q21;q23) MLL rearranged (WHO classification 2008)
CONSENSUS GROUP: ADDITIONAL INFORMATION/STUDIES
Additional immunostains performed by the conference consensus group:
CD19: Negative
CD79a: Negative
CONSENSUS DIAGNOSIS
Therapy related myeloid neoplasm, mixed phenotype acute leukemia, with t(4;11), MLL rearranged, with relapse as acute myeloid leukemia (monocytic differentiation)
| Blood smear (BM-1), Wright-Giemsa stain, x1000 |  |
| Bone marrow aspirate smear (BM-1), Wright-Giemsa stain, x400 |  |
| Blood smear (BM-2), Wright-Giemsa stain, x400 |  |
| Bone marrow aspirate smear (BM-2), Wright-Giemsa stain, x400 |  |
| Bone marrow core biopsy section (BM-1), H&E stain, x400 |  |
| Bone marrow core biopsy section (BM-1), TdT immunoperoxidase stain, x200 |  |
| Bone marrow core biopsy section (BM-1), CD68 immunoperoxidase stain, x200 | 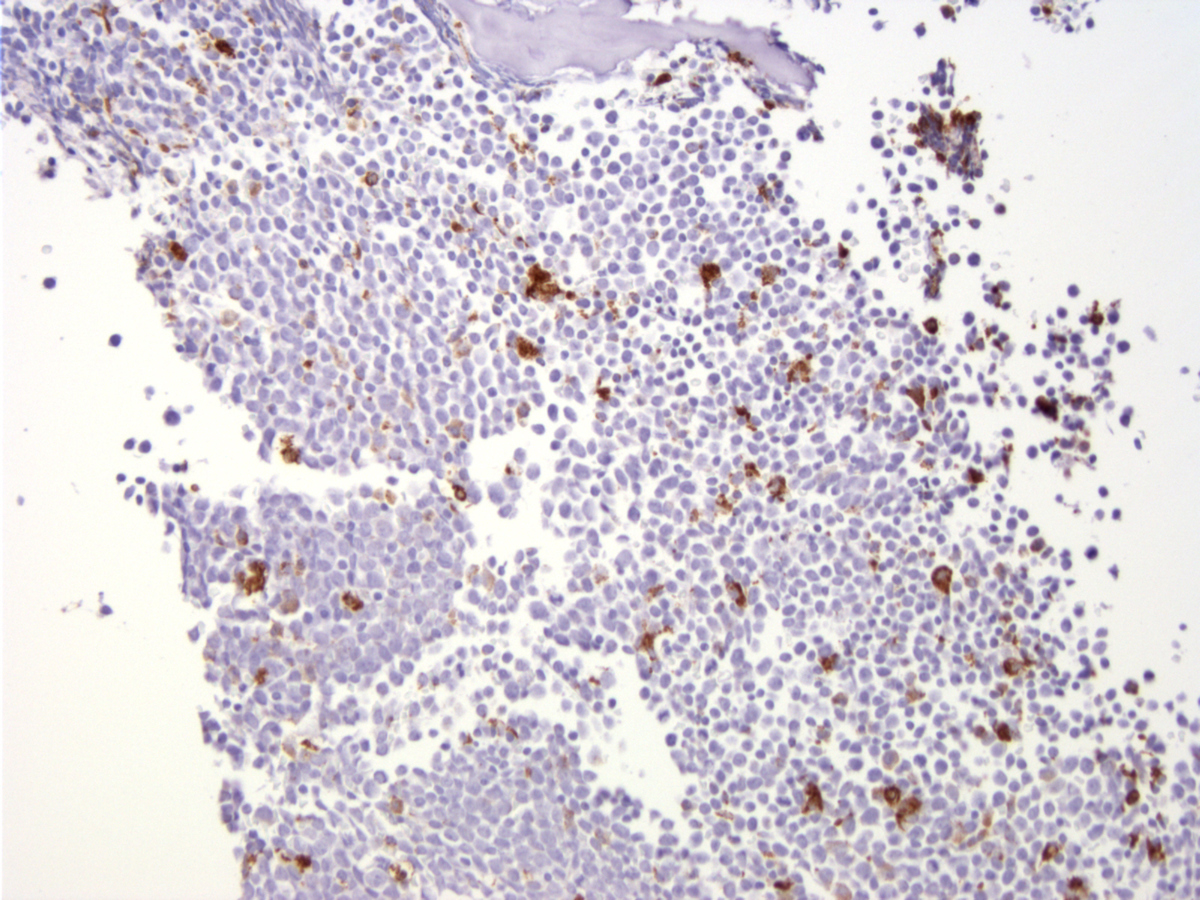 |
| Bone marrow core biopsy section (BM-2), H&E stain, x400 |  |
| Bone marrow core biopsy section (BM-2), TdT immunoperoxidase stain, x200 |  |
| Bone marrow core biopsy section (BM-2), CD68 immunoperoxidase stain, x200 |  |
| Bone marrow core biopsy section (BM-4), H&E stain, x400 |  |
| Bone marrow core biopsy section (BM-4), TdT immunoperoxidase stain, x200 |  |
| Bone marrow core biopsy section (BM-4), CD68 immunoperoxidase stain, x200 |  |